

Pulselessness After Initiation of Cardiopulmonary Resuscitation for Bradycardia in Hospitalized Children
- PMID: 31006260
- PMCID: PMC6663562
- DOI: 10.1161/CIRCULATIONAHA.118.039048
Pulselessness After Initiation of Cardiopulmonary Resuscitation for Bradycardia in Hospitalized Children
Abstract
Background: Cardiopulmonary resuscitation (CPR) is initiated in hospitalized children with bradycardia and poor perfusion. However, their rate of progression to pulseless cardiac arrest despite CPR and the differences in survival compared with initially pulseless arrest are unknown. We examined the prevalence and predictors of survival of children who progress from bradycardia to pulseless in-hospital cardiac arrest despite CPR.
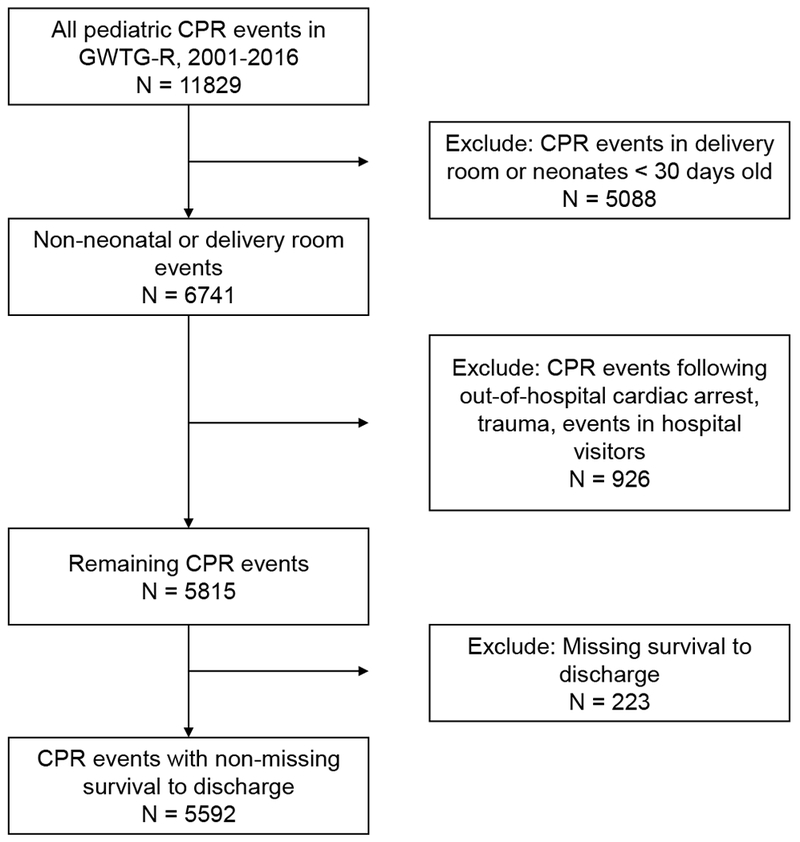
Methods: Pediatric patients >30 days and <18 years of age who received CPR at hospitals participating in Get With The Guidelines-Resuscitation during 2000 to 2016 were included. Each CPR event was classified as bradycardia with pulse, bradycardia with subsequent pulselessness, and initial pulseless cardiac arrest. We assessed risk-adjusted rates of survival to hospital discharge using multilevel Poisson regression models.
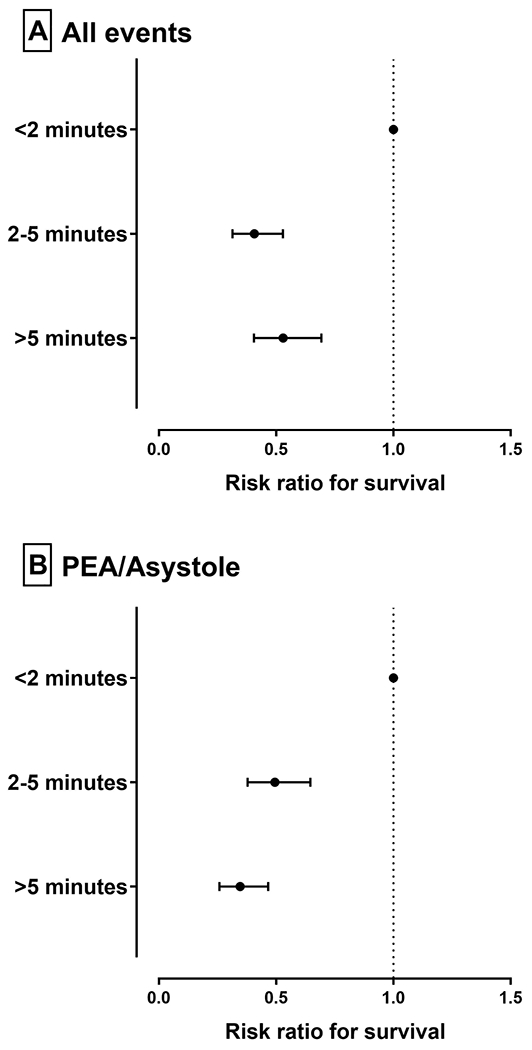
Results: Overall, 5592 pediatric patients were treated with CPR, of whom 2799 (50.1%) received CPR for bradycardia with poor perfusion and 2793 (49.9%) for initial pulseless cardiac arrest. Among those with bradycardia, 869 (31.0%, or 15.5% of cohort) became pulseless after a median of 3 minutes of CPR (interquartile range, 1-9 minutes). Rates of survival to discharge were 70.0% (1351 of 1930) for bradycardia with pulse, 30.1% (262 of 869) for bradycardia progressing to pulselessness, and 37.5% (1046 of 2793) for initial pulseless cardiac arrest (P for difference across groups <0.001). Children who became pulseless despite CPR for bradycardia had a 19% lower likelihood (risk ratio, 0.81 [95% CI, 0.70, 0.93]; P=0.004) of surviving to hospital discharge than those who were initially pulseless. Among children who progressed to pulselessness despite CPR for bradycardia, a longer interval between CPR and pulselessness was a predictor of lower survival (reference, <2 minutes; for 2-5 minutes, risk ratio, 0.54 [95% CI, 0.41-0.70]; for >5 minutes, risk ratio, 0.41 [95% CI, 0.32-0.53]).
Conclusions: Among hospitalized children in whom CPR is initiated, half have bradycardia with poor perfusion at the initiation of chest compressions, and nearly one-third of these progress to pulseless in-hospital cardiac arrest despite CPR. Survival was significantly lower for children who progress to pulselessness despite CPR compared with those who were initially pulseless. These findings suggest that pediatric patients who lose their pulse despite resuscitation attempts are at particularly high risk and require a renewed focus on postresuscitation care.
Keywords: advanced cardiac life support; bradycardia; critical care; pediatrics; resuscitation.
Figures
Similar articles
-
Survival and Hemodynamics During Pediatric Cardiopulmonary Resuscitation for Bradycardia and Poor Perfusion Versus Pulseless Cardiac Arrest.Crit Care Med. 2020 Jun;48(6):881-889. doi: 10.1097/CCM.0000000000004308. Crit Care Med. 2020. PMID: 32301844 Free PMC article.
-
Cardiopulmonary resuscitation for bradycardia with poor perfusion versus pulseless cardiac arrest.Pediatrics. 2009 Dec;124(6):1541-8. doi: 10.1542/peds.2009-0727. Epub 2009 Nov 16. Pediatrics. 2009. PMID: 19917587
-
Early bolus epinephrine administration during pediatric cardiopulmonary resuscitation for bradycardia with poor perfusion: an ICU-resuscitation study.Crit Care. 2024 Jul 16;28(1):242. doi: 10.1186/s13054-024-05018-7. Crit Care. 2024. PMID: 39010134 Free PMC article. Clinical Trial.
-
Chest Compressions for Bradycardia during Neonatal Resuscitation-Do We Have Evidence?Children (Basel). 2019 Oct 29;6(11):119. doi: 10.3390/children6110119. Children (Basel). 2019. PMID: 31671867 Free PMC article. Review.
-
2017 American Heart Association Focused Update on Pediatric Basic Life Support and Cardiopulmonary Resuscitation Quality: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.Circulation. 2018 Jan 2;137(1):e1-e6. doi: 10.1161/CIR.0000000000000540. Epub 2017 Nov 6. Circulation. 2018. PMID: 29114009 Review.
Cited by
-
Epidemiology and outcomes of infants after cardiopulmonary resuscitation in the neonatal or pediatric intensive care unit from a national registry.Resuscitation. 2021 Aug;165:14-22. doi: 10.1016/j.resuscitation.2021.05.029. Epub 2021 Jun 6. Resuscitation. 2021. PMID: 34107334 Free PMC article.
-
Survival outcomes of in-hospital cardiac arrest in pediatric patients in the USA.Eur J Pediatr. 2021 Aug;180(8):2513-2520. doi: 10.1007/s00431-021-04082-3. Epub 2021 Apr 26. Eur J Pediatr. 2021. PMID: 33899153
-
[Paediatric Life Support].Notf Rett Med. 2021;24(4):650-719. doi: 10.1007/s10049-021-00887-9. Epub 2021 Jun 2. Notf Rett Med. 2021. PMID: 34093080 Free PMC article. Review. German.
-
Association of Pentachlorophenol with Fetal Risk of Prolonged Bradycardia: A Systematic Review and Meta-Analysis.J Healthc Eng. 2022 Mar 27;2022:7552294. doi: 10.1155/2022/7552294. eCollection 2022. J Healthc Eng. 2022. Retraction in: J Healthc Eng. 2023 Aug 16;2023:9807423. doi: 10.1155/2023/9807423. PMID: 35388327 Free PMC article. Retracted.
-
Trends in Survival After Pediatric In-Hospital Cardiac Arrest in the United States.Circulation. 2019 Oct 22;140(17):1398-1408. doi: 10.1161/CIRCULATIONAHA.119.041667. Epub 2019 Sep 23. Circulation. 2019. PMID: 31542952 Free PMC article.
References
-
- Berg MD, Nadkarni VM, Zuercher M and Berg RA. In-hospital pediatric cardiac arrest. Pediatr Clin North Am 2008;55:589–604, x. - PubMed
-
- Morrison LJ, Neumar RW, Zimmerman JL, Link MS, Newby LK, McMullan PW Jr., Hoek TV, Halverson CC, Doering L, Peberdy MA, Edelson DP, American Heart Association Emergency Cardiovascular Care Committee CoCCCP, Resuscitation CoC, Stroke Nursing CoCC and Council on P. Strategies for improving survival after in-hospital cardiac arrest in the United States: 2013 consensus recommendations: a consensus statement from the American Heart Association. Circulation. 2013;127:1538–1563. - PubMed
-
- Nadkarni VM, Larkin GL, Peberdy MA, Carey SM, Kaye W, Mancini ME, Nichol G, Lane-Truitt T, Potts J, Omato JP, Berg RA and National Registry of Cardiopulmonary Resuscitation I. First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults. JAMA. 2006;295:50–57. - PubMed
-
- de Caen AR, Berg MD, Chameides L, Gooden CK, Hickey RW, Scott HF, Sutton RM, Tijssen JA, Topjian A, van der Jagt EW, Schexnayder SM and Samson RA. Part 12: Pediatric Advanced Life Support: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015;132:S526–S542. - PMC - PubMed
