

Local Conduction Velocity in the Presence of Late Gadolinium Enhancement and Myocardial Wall Thinning: A Cardiac Magnetic Resonance Study in a Swine Model of Healed Left Ventricular Infarction
- PMID: 31006313
- PMCID: PMC6613809
- DOI: 10.1161/CIRCEP.119.007175
Local Conduction Velocity in the Presence of Late Gadolinium Enhancement and Myocardial Wall Thinning: A Cardiac Magnetic Resonance Study in a Swine Model of Healed Left Ventricular Infarction
Abstract
Background: Conduction velocity (CV) is an important property that contributes to the arrhythmogenicity of the tissue substrate. The aim of this study was to investigate the association between local CV versus late gadolinium enhancement (LGE) and myocardial wall thickness in a swine model of healed left ventricular infarction.
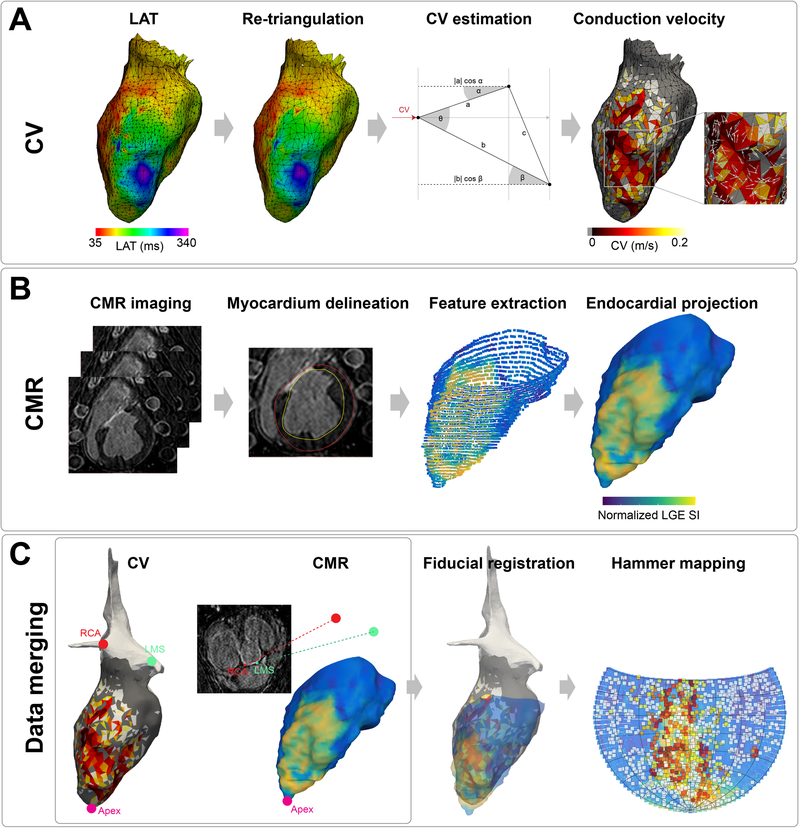
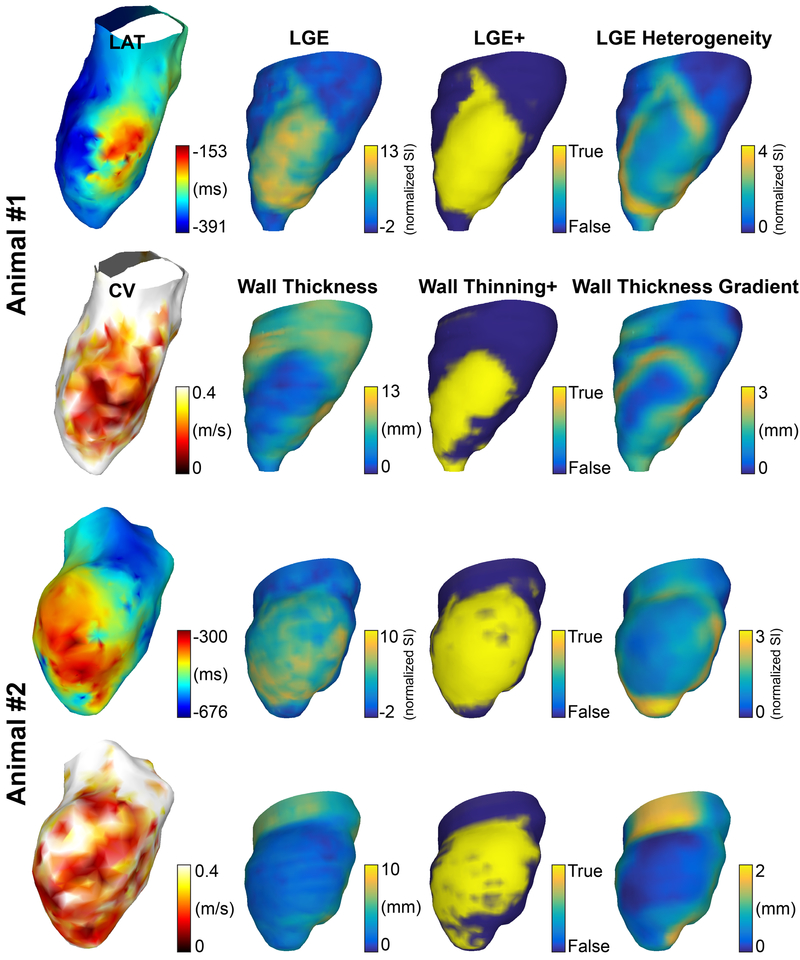
Methods: Six swine with healed myocardial infarction underwent cardiovascular magnetic resonance imaging and electroanatomic mapping. Two healthy controls (one treated with amiodarone and one unmedicated) underwent electroanatomic mapping with identical protocols to establish the baseline CV. CV was estimated using a triangulation technique. LGE+ regions were defined as signal intensity >2 SD than the mean of remote regions, wall thinning+ as those with wall thickness <2 SD than the mean of remote regions. LGE heterogeneity was defined as SD of LGE in the local neighborhood of 5 mm and wall thickness gradient as SD within 5 mm. Cardiovascular magnetic resonance and electroanatomic mapping data were registered, and hierarchical modeling was performed to estimate the mean difference of CV (LGE+/-, wall thinning+/-), or the change of the mean of CV per unit change (LGE heterogeneity, wall thickness gradient).
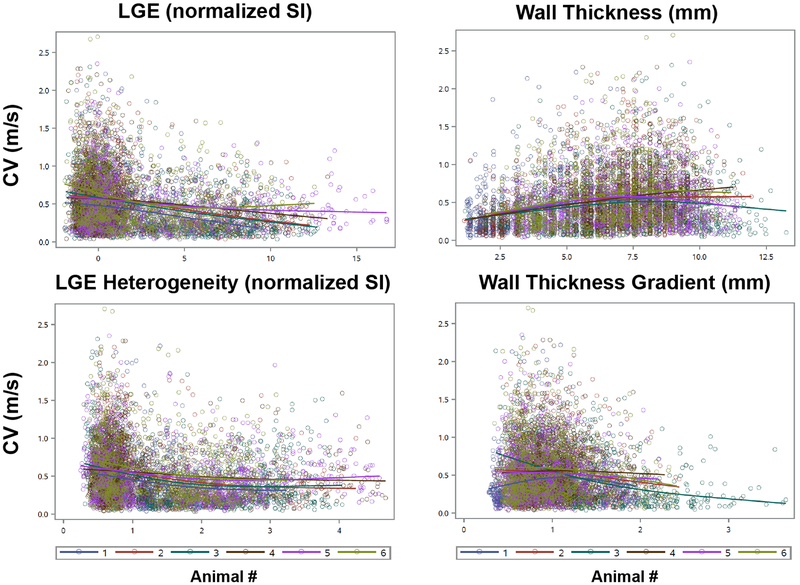
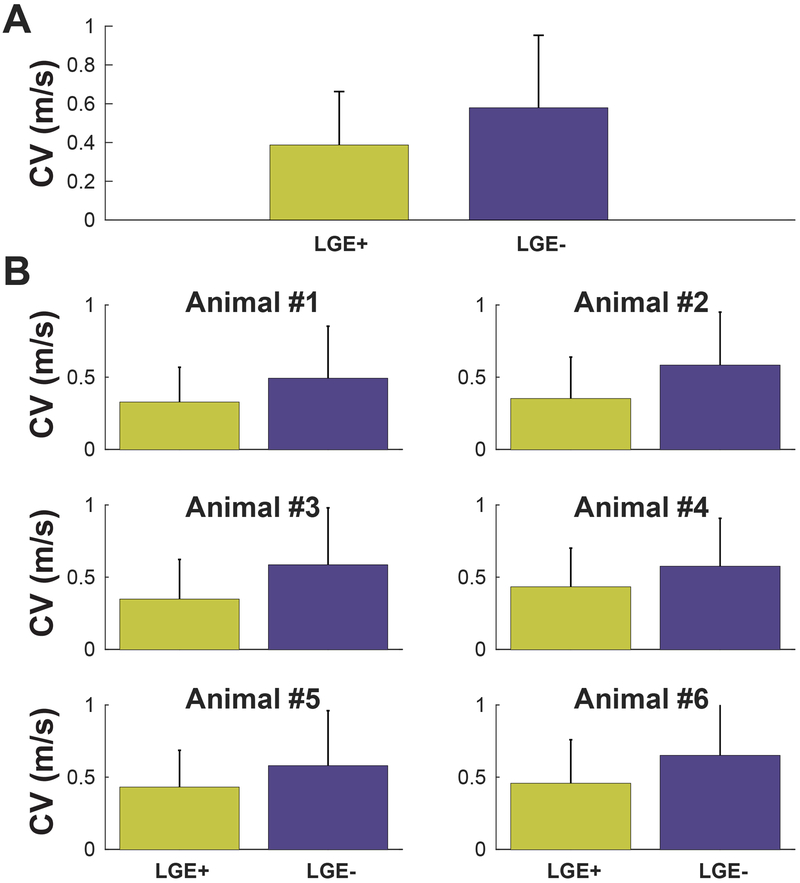
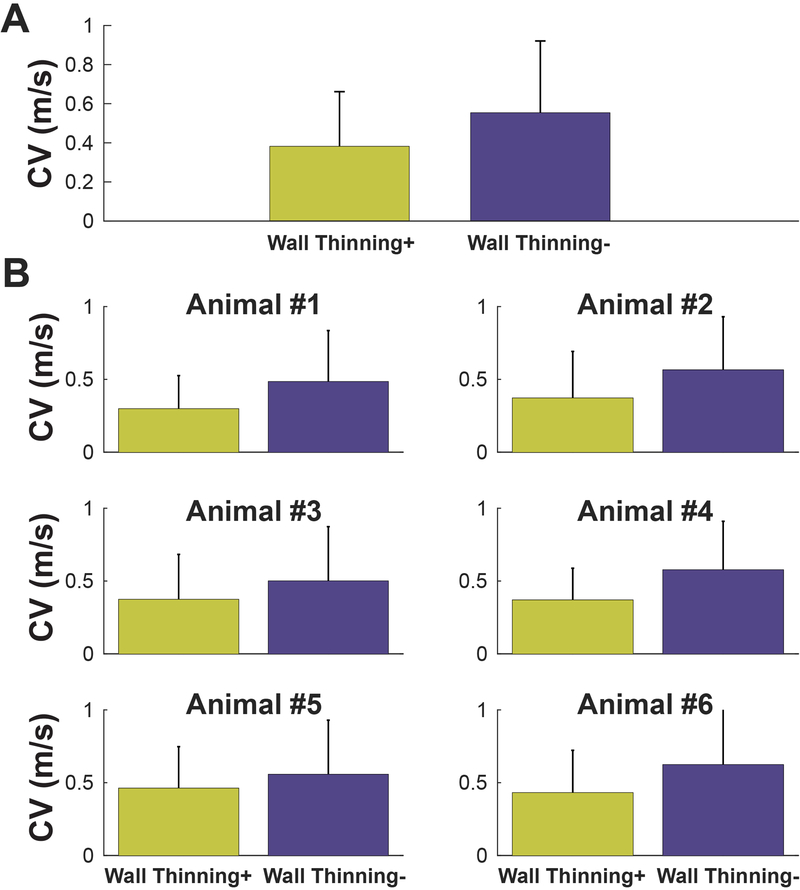
Results: Significantly slower CV was observed in LGE+ (0.33±0.25 versus 0.54±0.36 m/s; P<0.001) and wall thinning+ regions (0.38±0.28 versus 0.55±0.37 m/s; P<0.001). Areas with greater LGE heterogeneity ( P<0.001) and wall thickness gradient ( P<0.001) exhibited slower CV.
Conclusions: Slower CV is observed in the presence of LGE, myocardial wall thinning, high LGE heterogeneity, and a high wall thickness gradient. Cardiovascular magnetic resonance may offer a valuable imaging surrogate for estimating CV, which may support noninvasive identification of the arrhythmogenic substrate.
Keywords: conduction velocity; electroanatomic mapping; late gadolinium enhancement; magnetic resonance imaging; myocardial infarction; myocardial wall thickness; ventricular tachycardia.
Figures

Similar articles
-
Accurate Conduction Velocity Maps and Their Association With Scar Distribution on Magnetic Resonance Imaging in Patients With Postinfarction Ventricular Tachycardias.Circ Arrhythm Electrophysiol. 2020 Apr;13(4):e007792. doi: 10.1161/CIRCEP.119.007792. Epub 2020 Mar 19. Circ Arrhythm Electrophysiol. 2020. PMID: 32191131 Free PMC article.
-
Implications of bipolar voltage mapping and magnetic resonance imaging resolution in biventricular scar characterization after myocardial infarction.Europace. 2019 Jan 1;21(1):163-174. doi: 10.1093/europace/euy192. Europace. 2019. PMID: 30239689 Free PMC article.
-
Association of Left Atrial Local Conduction Velocity With Late Gadolinium Enhancement on Cardiac Magnetic Resonance in Patients With Atrial Fibrillation.Circ Arrhythm Electrophysiol. 2016 Mar;9(3):e002897. doi: 10.1161/CIRCEP.115.002897. Circ Arrhythm Electrophysiol. 2016. PMID: 26917814 Free PMC article.
-
Myocardial Fibrosis Assessment by LGE Is a Powerful Predictor of Ventricular Tachyarrhythmias in Ischemic and Nonischemic LV Dysfunction: A Meta-Analysis.JACC Cardiovasc Imaging. 2016 Sep;9(9):1046-1055. doi: 10.1016/j.jcmg.2016.01.033. Epub 2016 Jul 20. JACC Cardiovasc Imaging. 2016. PMID: 27450871 Review.
-
Applications of cardiac magnetic resonance in electrophysiology.Circ Arrhythm Electrophysiol. 2009 Feb;2(1):63-71. doi: 10.1161/CIRCEP.108.811562. Circ Arrhythm Electrophysiol. 2009. PMID: 19808444 Free PMC article. Review.
Cited by
-
Mapping of ventricular tachycardia in patients with ischemic cardiomyopathy: Current approaches and future perspectives.Clin Cardiol. 2019 Oct;42(10):1041-1050. doi: 10.1002/clc.23245. Epub 2019 Aug 14. Clin Cardiol. 2019. PMID: 31411347 Free PMC article. Review.
-
A Computational Study of the Electrophysiological Substrate in Patients Suffering From Atrial Fibrillation.Front Physiol. 2021 Jul 8;12:673612. doi: 10.3389/fphys.2021.673612. eCollection 2021. Front Physiol. 2021. PMID: 34305637 Free PMC article.
-
Activation During Sinus Rhythm in Ventricles With Healed Infarction: Differentiation Between Arrhythmogenic and Nonarrhythmogenic Scar.Circ Arrhythm Electrophysiol. 2019 Oct;12(10):e007879. doi: 10.1161/CIRCEP.119.007879. Epub 2019 Oct 10. Circ Arrhythm Electrophysiol. 2019. PMID: 31597477 Free PMC article.
-
Accurate Conduction Velocity Maps and Their Association With Scar Distribution on Magnetic Resonance Imaging in Patients With Postinfarction Ventricular Tachycardias.Circ Arrhythm Electrophysiol. 2020 Apr;13(4):e007792. doi: 10.1161/CIRCEP.119.007792. Epub 2020 Mar 19. Circ Arrhythm Electrophysiol. 2020. PMID: 32191131 Free PMC article.
-
Late Gadolinium Enhancement Cardiovascular Magnetic Resonance Assessment of Substrate for Ventricular Tachycardia With Hemodynamic Compromise.Front Cardiovasc Med. 2021 Oct 26;8:744779. doi: 10.3389/fcvm.2021.744779. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34765656 Free PMC article.
References
-
- Chow AWC, Schilling RJ, Davies DW, Peters NS. Characteristics of wavefront propagation in reentrant circuits causing human ventricular tachycardia. Circulation. 2002;105:2172–2178. - PubMed
-
- Josephson ME, Horowitz LN, Farshidi A. Continuous local electrical activity. A mechanism of recurrent ventricular tachycardia. Circulation. 1978;57:659–665. - PubMed
-
- Josephson ME, Horowitz LN, Farshidi A, Spielman SR, Michelson EL, Greenspan AM. Sustained ventricular tachycardia: Evidence for protected localized reentry. Am J Cardiol. 1978;42:416–424. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
