

Strain- and Species-Level Variation in the Microbiome of Diabetic Wounds Is Associated with Clinical Outcomes and Therapeutic Efficacy
- PMID: 31006638
- PMCID: PMC6526540
- DOI: 10.1016/j.chom.2019.03.006
Strain- and Species-Level Variation in the Microbiome of Diabetic Wounds Is Associated with Clinical Outcomes and Therapeutic Efficacy
Abstract
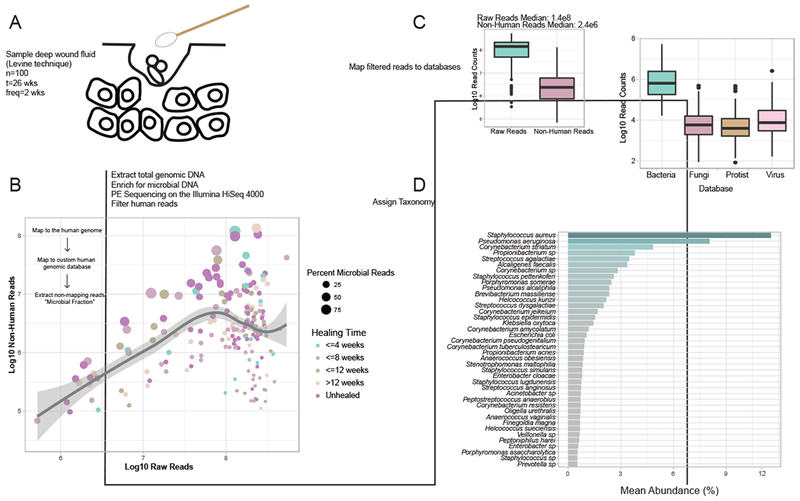
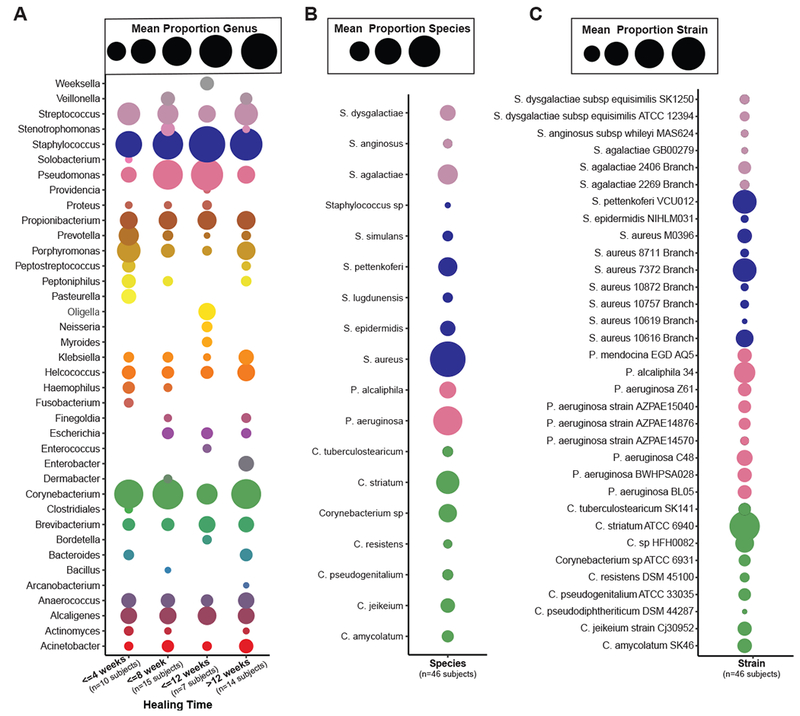
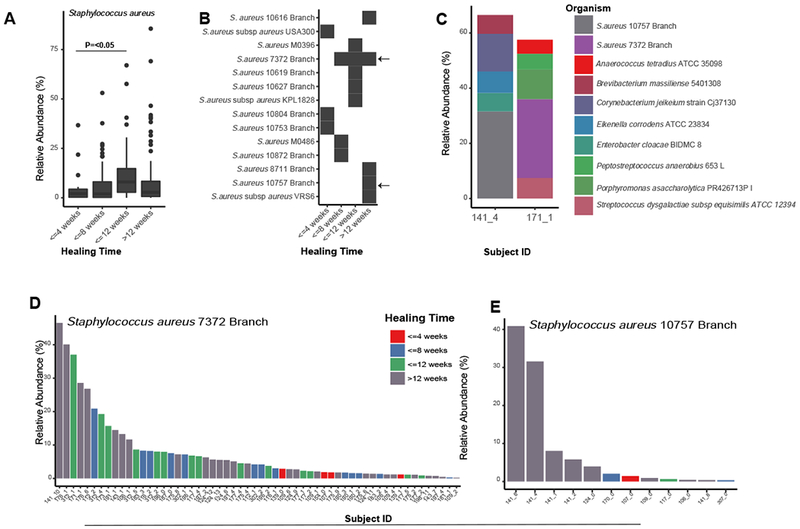
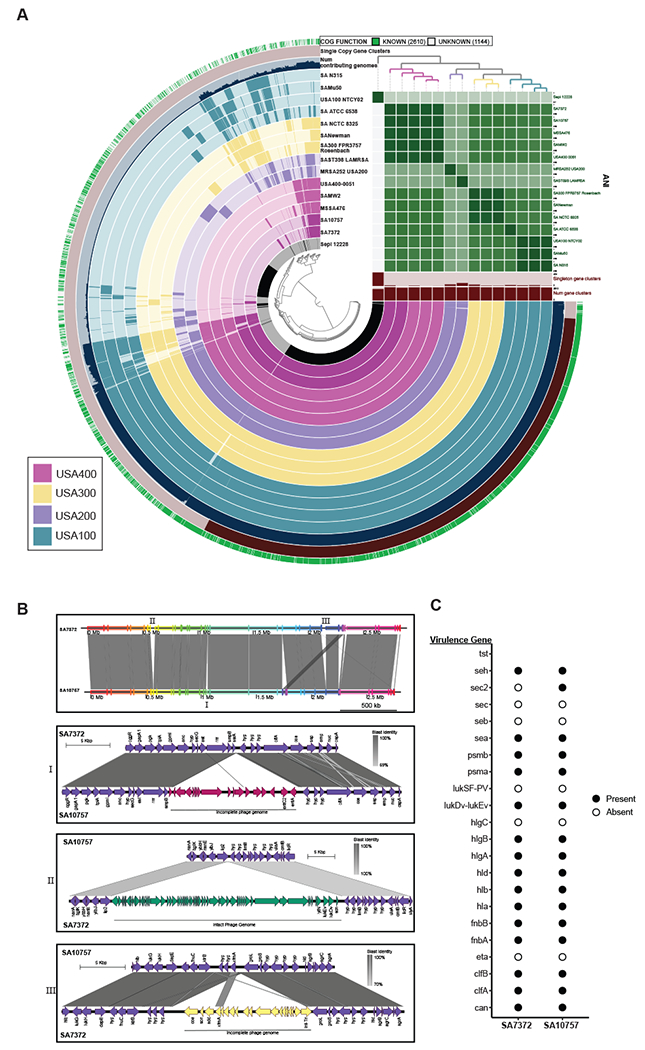
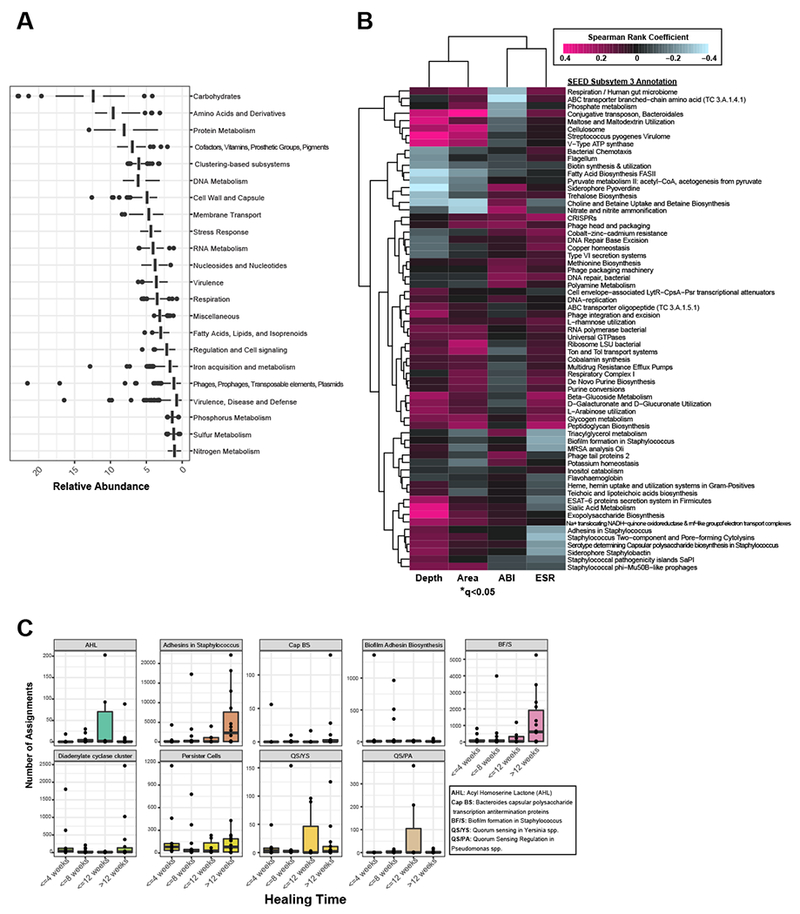
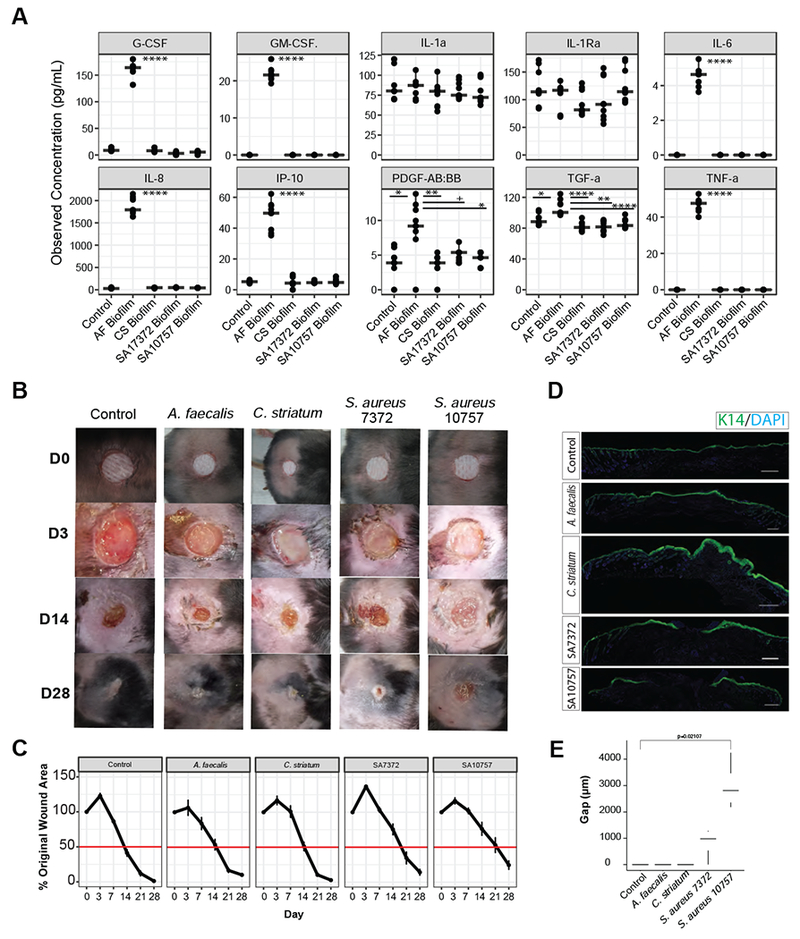
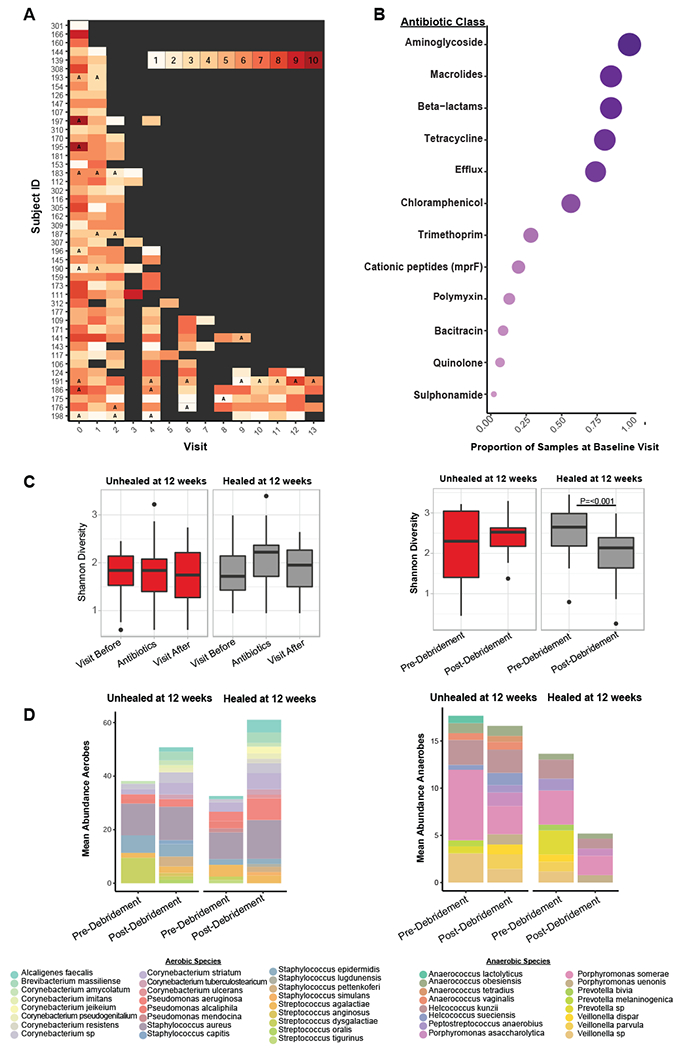
Chronic wounds are a major complication of diabetes associated with high morbidity and health care expenditures. To investigate the role of colonizing microbiota in diabetic wound healing, clinical outcomes, and response to interventions, we conducted a longitudinal, prospective study of patients with neuropathic diabetic foot ulcers (DFU). Metagenomic shotgun sequencing revealed that strain-level variation of Staphylococcus aureus and genetic signatures of biofilm formation were associated with poor outcomes. Cultured wound isolates of S. aureus elicited differential phenotypes in mouse models that corresponded with patient outcomes, while wound "bystanders" such as Corynebacterium striatum and Alcaligenes faecalis, typically considered commensals or contaminants, also significantly impacted wound severity and healing. Antibiotic resistance genes were widespread, and debridement, rather than antibiotic treatment, significantly shifted the DFU microbiota in patients with more favorable outcomes. These findings suggest that the DFU microbiota may be a marker for clinical outcomes and response to therapeutic interventions.
Keywords: antibiotic resistance; chronic wounds; diabetes; metagenomics; microbiome; wound healing.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
DECLARATION OF INTERESTS
The authors have no competing interests to declare.
Figures
Comment in
-
Bad "Staph" in the Wound Environment of Diabetic Foot Ulcers.Cell Host Microbe. 2019 May 8;25(5):638-640. doi: 10.1016/j.chom.2019.04.006. Cell Host Microbe. 2019. PMID: 31071293
References
-
- Armstrong DG, Wrobel J, and Robbins JM (2007). Guest Editorial: are diabetes-related wounds and amputations worse than cancer? Int Wound J 4, 286–287. - PubMed
-
- Arwert EN, Hoste E, and Watt FM (2012). Epithelial stem cells, wound healing and cancer. Nat Rev Cancer 12, 170–180. - PubMed
-
- Ashrafi M, Sebastian A, Shih B, Greaves N, Alonso-Rasgado T, Baguneid M, and Bayat A (2016). Whole genome microarray data of chronic wound debridement prior to application of dermal skin substitutes. Wound Repair Regen 24, 870–875. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
