

Glue-assisted retinopexy for rhegmatogenous retinal detachments (GuARD): A novel surgical technique for closing retinal breaks
- PMID: 31007238
- PMCID: PMC6498943
- DOI: 10.4103/ijo.IJO_1943_18
Glue-assisted retinopexy for rhegmatogenous retinal detachments (GuARD): A novel surgical technique for closing retinal breaks
Abstract
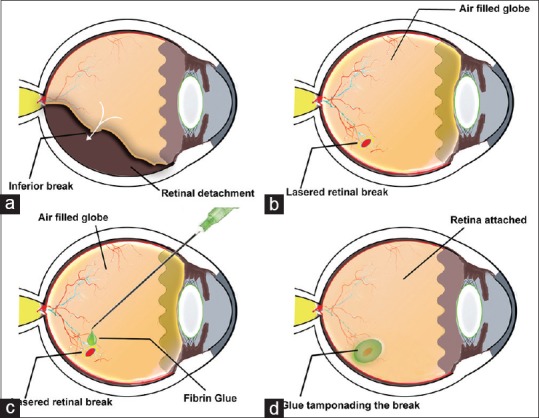
Purpose: This study describes a novel surgical technique of fibrin glue-assisted retinopexy for rhegmatogenous retinal detachment (GuARD) without oil or gas tamponade after pars plana vitrectomy (PPV).
Methods: This pilot clinical trial included five eyes of five patients with rhegmatogenous retinal detachments (RD). A complete PPV was done in all cases followed by fluid-air exchange, laser photocoagulation around the break/s, and application of 0.1-0.2 mL of fibrin glue. No air, long-acting gas or silicone oil was used subsequently. No specific postoperative positioning was prescribed. The primary outcome measure was efficacy of the procedure defined as successful anatomical retinal reattachment. Secondary outcome measures were postoperative improvement in best corrected visual acuity (BCVA) and complications.
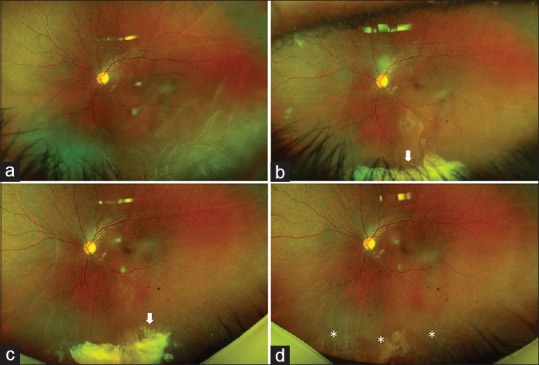
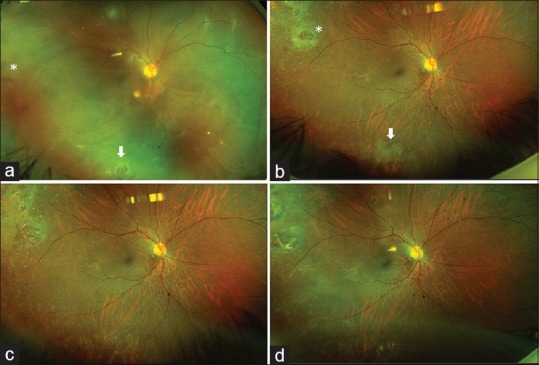
Results: The median age of patients was 55 (range: 36-61 years) years and median duration of symptoms was 15 (range: 7-60) days. All eyes were pseudophakic, four eyes had inferior and one eye had total RD. Successful retinal reattachment was achieved in all (100%) cases and was maintained at the end of 3-8 months of follow-up. The median BCVA improved from 20/100 preoperatively to 20/80 at 1-week and 20/50 at 1-month postoperatively. None of the eyes had any postoperative complications such as elevated intraocular pressures or unexpected inflammation.
Conclusion: The findings of this study suggest that GuARD is a promising technique for treatment of rhegmatogenous RD that may allow early visual recovery while avoiding the problems of gas or oil tamponade and obviating the need of postoperative positioning.
Keywords: Fibrin glue; retinal detachment surgery; rhegmatogenous retinal detachment.
Conflict of interest statement
None
Figures
Comment in
-
Commentary: Sealing breaks comfortably- A novel approach to retinopexy without positioning.Indian J Ophthalmol. 2019 May;67(5):681. doi: 10.4103/ijo.IJO_269_19. Indian J Ophthalmol. 2019. PMID: 31007239 Free PMC article. No abstract available.
-
Commentary: Fibrin sealant for temporary retinopexy.Indian J Ophthalmol. 2019 May;67(5):682-683. doi: 10.4103/ijo.IJO_67_19. Indian J Ophthalmol. 2019. PMID: 31007240 Free PMC article. No abstract available.
-
Commentary: Fibrin glue in rhegmatogenous retinal detachment repair-Are we there yet?Indian J Ophthalmol. 2019 May;67(5):683-684. doi: 10.4103/ijo.IJO_104_19. Indian J Ophthalmol. 2019. PMID: 31007241 Free PMC article. No abstract available.
References
-
- Adelman RA, Parnes AJ, Ducournau D. Strategy for the management of uncomplicated retinal detachments: The European vitreo-retinal society retinal detachment study report 1. Ophthalmology. 2013;20:1804–08. - PubMed
-
- Heimann H, Bartz-Schmidt KU, Bornfeld N, Weiss C, Hilgers RD, Foerster MH, et al. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment: A prospective randomized multicenter clinical study. Ophthalmology. 2007;114:2142–54. - PubMed
-
- Chong DY, Fuller DG. The declining use of scleral buckling with vitrectomy for primary retinal detachments. Arch Ophthalmol. 2010;128:1206–7. - PubMed
-
- Barr CC, Lai MY, Lean JS, Linton KL, Trese M, Abrams G, et al. Postoperative intraocular pressure abnormalities in the silicone study. Silicone study report 4. Ophthalmology. 1993;100:1629–35. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
