

Fusarium infection-induced partial failure of free anterolateral thigh musculocutaneous flap: Case report
- PMID: 31007923
- PMCID: PMC6457015
- DOI: 10.1177/2050313X19841963
Fusarium infection-induced partial failure of free anterolateral thigh musculocutaneous flap: Case report
Abstract
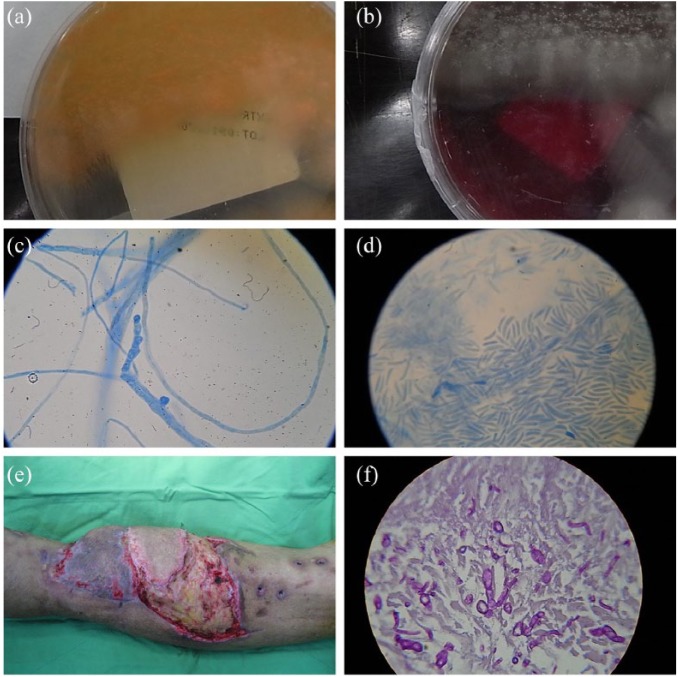
Fusarium species, a soil-borne fungi, causes disease in animals and humans, particularly in immunocompromized patients. A 62-year-old male presented with type II diabetes mellitus, diagnosed 4 years ago. He had a motorcycle accident-caused open tibiofibular fracture of the left lower extremity (Gustilo grade IIIb). With open reduction and internal fixation, an anterolateral thigh musculocutaneous flap was harvested for coverage of exposed bone and defect reconstruction. Partial failure of the flap occurred 9 days following reconstruction, and histological examination revealed Fusarium spp. After treatment with antifungal drugs and debridement, we performed a split-thickness skin graft. At 2-year follow-up, the flap was viable with adequate bone union. This is the first reported case of partial flap failure due to a Fusarium spp. infection. Possibility of fungal infections in patients with late-onset flap failure should be noted. Prompt diagnosis and treatment are needed to prevent repeated free-tissue transfer and/or devastating outcomes.
Keywords: Fusarium infection; anterolateral thigh flap; open tibiofibular fracture.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Figures


Similar articles
-
Outcomes of anterolateral thigh-free flaps and conversion from external to internal fixation with bone grafting in gustilo type IIIB open tibial fractures.Microsurgery. 2012 Sep;32(6):431-7. doi: 10.1002/micr.21970. Epub 2012 Mar 21. Microsurgery. 2012. PMID: 22434519
-
One-stage treatment and reconstruction of Gustilo Type III open tibial shaft fractures with a vascularized fibular osteoseptocutaneous flap graft.J Orthop Trauma. 2010 Dec;24(12):745-51. doi: 10.1097/BOT.0b013e3181d88a07. J Orthop Trauma. 2010. PMID: 21063216
-
Free anterolateral thigh adipofascial perforator flap.Plast Reconstr Surg. 2003 Sep 15;112(4):976-82. doi: 10.1097/01.PRS.0000076221.25738.66. Plast Reconstr Surg. 2003. PMID: 12973212
-
An ideal and versatile material for soft-tissue coverage: experiences with most modifications of the anterolateral thigh flap.J Reconstr Microsurg. 2004 Jul;20(5):377-83. doi: 10.1055/s-2004-830003. J Reconstr Microsurg. 2004. PMID: 15237357
-
On Partial Fracture of the Neck of the Thigh-Bone.Med Chir Rev. 1845 Jan;1(1):80-81. Med Chir Rev. 1845. PMID: 29918979 Free PMC article. Review. No abstract available.
Cited by
-
Latissimus dorsi musculocutaneous flap grafting to the infected recipient site in a patient with irradiated locally advanced breast cancer and multiple lung metastases.Surg Case Rep. 2023 Jul 10;9(1):127. doi: 10.1186/s40792-023-01711-x. Surg Case Rep. 2023. PMID: 37428338 Free PMC article.
-
Clinical spectrum of fusariosis from a tertiary care center in India- a retrospective study.Iran J Microbiol. 2024 Feb;16(1):145-150. doi: 10.18502/ijm.v16i1.14884. Iran J Microbiol. 2024. PMID: 38682054 Free PMC article.
References
-
- Hay RJ. Fusarium infections of the skin. Curr Opin Infect Dis 2007; 20: 115–117. - PubMed
-
- Nucci M, Anaissie E. Cutaneous infection by Fusarium species in healthy and immunocompromised hosts: implications for diagnosis and management. Clin Infect Dis 2002; 35(8): 909–920. - PubMed
-
- Boutati EI, Anaissie EJ. Fusarium, a significant emerging pathogen in patients with hematologic malignancy: ten years’ experience at a cancer center and implications for management. Blood 1997; 90(3): 999–1008. - PubMed
-
- Dignani MC, Anaissie E. Human fusariosis. Clin Microbiol Infect 2004; 10(Suppl. 1): 67–75. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
