

Minor stroke due to large artery occlusion. When is intravenous thrombolysis not enough? Results from the SITS International Stroke Thrombolysis Register
- PMID: 31008335
- PMCID: PMC6453245
- DOI: 10.1177/2396987317746003
Minor stroke due to large artery occlusion. When is intravenous thrombolysis not enough? Results from the SITS International Stroke Thrombolysis Register
Abstract
Purpose: Beyond intravenous thrombolysis, evidence is lacking on acute treatment of minor stroke caused by large artery occlusion. To identify candidates for additional endovascular therapy, we aimed to determine the frequency of non-haemorrhagic early neurological deterioration in patients with intravenous thrombolysis-treated minor stroke caused by occlusion of large proximal and distal cerebral arteries. Secondary aims were to establish risk factors for non-haemorrhagic early neurological deterioration and report three-month outcomes in patients with and without non-haemorrhagic early neurological deterioration.
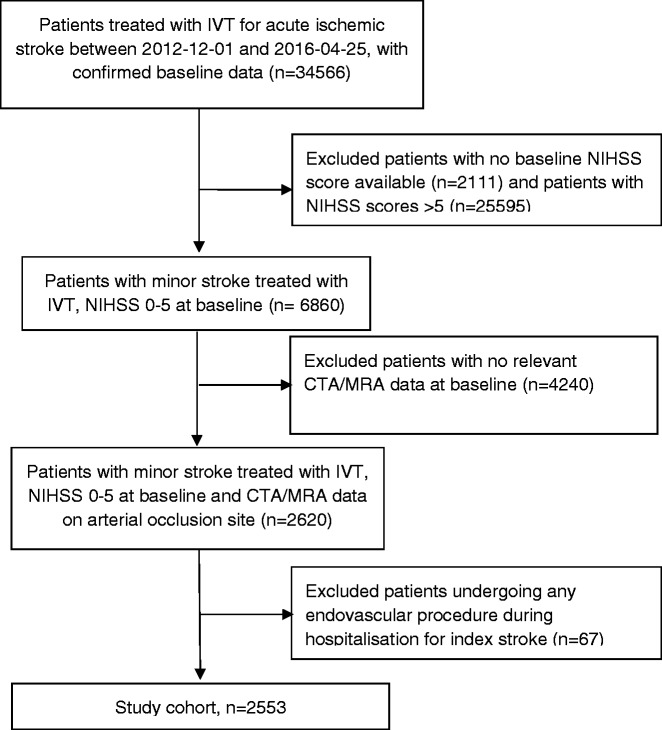
Method: We analysed data from the SITS International Stroke Thrombolysis Register on 2553 patients with intravenous thrombolysis-treated minor stroke (NIH Stroke Scale scores 0-5) and available arterial occlusion data. Non-haemorrhagic early neurological deterioration was defined as an increase in NIH Stroke Scale score ≥4 at 24 h, without parenchymal hematoma on follow-up imaging within 22-36 h.
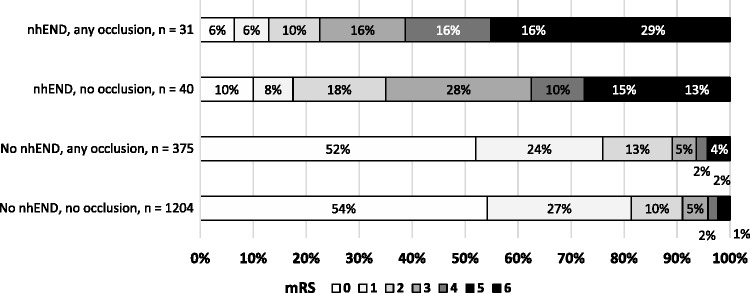
Findings: The highest frequency of non-haemorrhagic early neurological deterioration was seen in 30% of patients with terminal internal carotid artery or tandem occlusions (internal carotid artery + middle cerebral artery) (adjusted odds ratio: 10.3 (95% CI 4.3-24.9), p < 0.001) and 17% in extracranial carotid occlusions (adjusted odds ratio 4.3 (2.5-7.7), p < 0.001) versus 3.1% in those with no occlusion. Proximal middle cerebral artery-M1 occlusions had non-haemorrhagic early neurological deterioration in 9% (adjusted odds ratio 2.1 (0.97-4.4), p = 0.06). Among patients with any occlusion and non-haemorrhagic early neurological deterioration, 77% were dead or dependent at three months.
Conclusions: Patients with minor stroke caused by internal carotid artery occlusion, with or without tandem middle cerebral artery involvement, are at high risk of disabling deterioration, despite intravenous thrombolysis treatment. Acute vessel imaging contributes usefully even in minor stroke to identify and consider endovascular treatment, or intensive monitoring at a comprehensive stroke centre, for patients at high risk of neurological deterioration.
Keywords: Cerebral infarct; stroke management; stroke severity; thrombolysis.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MVM is the International Network and Research Executive of SITS International, which receives a grant from Boehringer Ingelheim for the SITS-ISTR. KRL has received fees and expenses from Boehringer Ingelheim for lectures and for serving on data monitoring committees. GAF has received lecture fees from Boehringer Ingelheim. CC, TM, MB, LS, and VS have no conflicting interests. SF has received a lecture fee from Boehringer Ingelheim. DT is a member of an Advisory Board (regarding Dabigatran) and has received speaker honoraria from Boehringer Ingelheim. NW is the Chairman of SITS International, which receives a grant from Boehringer Ingelheim for the SITS-ISTR. He has received fees and expenses for lectures and consultancies from Boehringer Ingelheim. NA is the Vice Chairman of SITS International, which receives a grant from Boehringer Ingelheim for the SITS-ISTR.
Figures
References
-
- Kharitonova T, Ahmed N, Thoren M, et al. Hyperdense middle cerebral artery sign on admission CT scan – prognostic significance for ischaemic stroke patients treated with intravenous thrombolysis in the safe implementation of thrombolysis in stroke international stroke thrombolysis register. Cerebrovasc Dis 2009; 27: 51–59. - PubMed
-
- Cooray C, Fekete K, Mikulik R, et al. Threshold for NIH stroke scale in predicting vessel occlusion and functional outcome after stroke thrombolysis. Int J Stroke 2015; 10: 822–829. - PubMed
-
- Heldner MR, Jung S, Zubler C, et al. Outcome of patients with occlusions of the internal carotid artery or the main stem of the middle cerebral artery with NIHSS score of less than 5: comparison between thrombolysed and non-thrombolysed patients. J Neurol Neurosurg Psychiatry 2015; 86: 755–760. - PubMed
LinkOut - more resources
Full Text Sources
