

The utility of ESR, CRP and platelets in the diagnosis of GCA
- PMID: 31008443
- PMCID: PMC6456976
- DOI: 10.1186/s41927-019-0061-z
The utility of ESR, CRP and platelets in the diagnosis of GCA
Abstract
Background: To compare the utility of ESR, CRP and platelets for the diagnosis of GCA.
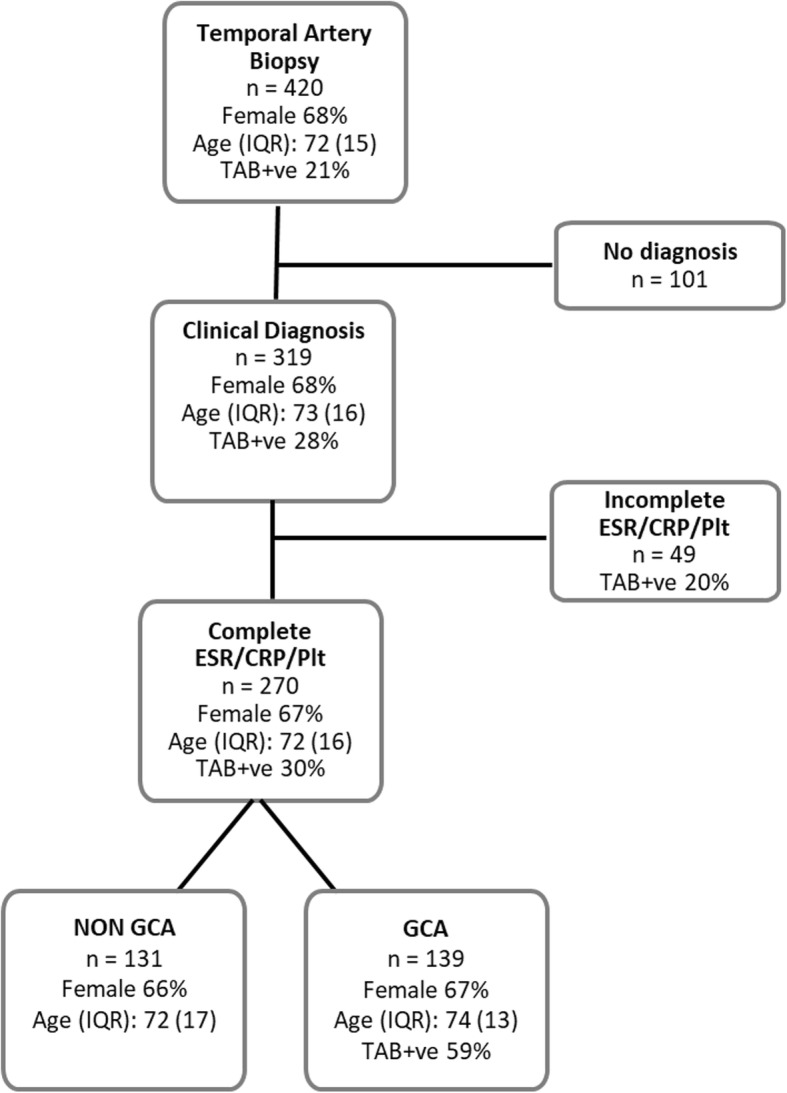
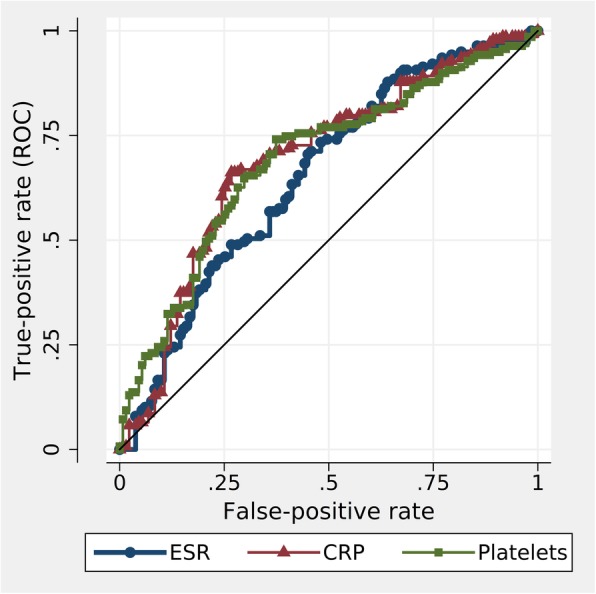
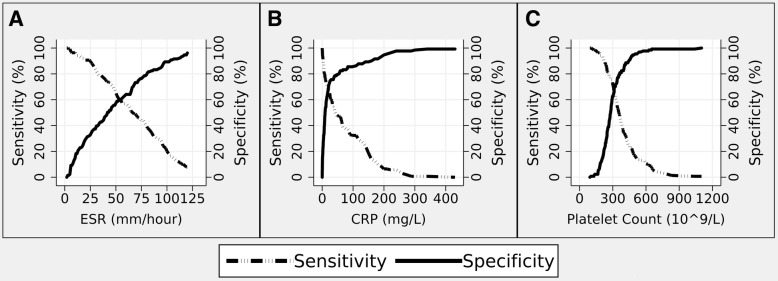
Method: A clinical diagnosis of GCA was determined by case-note review of 270 individuals (68% female, mean age 72 years) referred to a central pathology service for a temporal artery biopsy between 2011 and 2014. The highest levels of ESR, CRP and platelets (within 2 weeks of diagnosis) were documented. Evaluation of ESR, CRP and platelets for the diagnosis of GCA were compared using Receiver Operating Characteristic Area Under the Curve (ROC-AUC), and sensitivity/specificity at optimum cut-off values.
Results: GCA was clinically diagnosed in 139 (67%) patients, with 81 TAB positive. The AUC estimates for ESR, CRP and platelets were comparable (0.65 vs 0.72 vs 0.72, p = 0.08). The estimated optimal cut-off levels were confirmed at 50 mm/hour for ESR, and determined as 20 mg/L for CRP and 300 × 109/L for platelets. Sensitivity estimates for these three tests were comparable (p = 0.45) and ranged between 66% for ESR and 71% for platelets. Specificity estimates were also comparable (p = 0.11) and ranged between 57% for ESR and 68% for CRP. There was only moderate agreement between the three positive tests (agreement 67%, kappa: 0.34), and when considered collectively, CRP and platelet positive tests were independent predictors of GCA (p < 0.001), but the ESR was not (p = 0.76).
Conclusion: ESR, CRP and platelets are moderate, equivalent diagnostic tests for GCA, but may yield disparate results in individual patients. A combination of CRP and platelet tests may provide the best diagnostic utility for GCA.
Keywords: Diagnosis; Giant cell arteritis; Inflammatory markers; Vasculitis.
Conflict of interest statement
This study has obtained appropriate ethics approval for data collection, storage and publication via Southern Adelaide Clinical Human Research Ethics Committee (South Australia, Australia) with the approval number of 354.09. The need for informed consent was waived by the aforementioned ethics committee.Not applicable.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Role of thrombocytosis in diagnosis of giant cell arteritis and differentiation of arteritic from non-arteritic anterior ischemic optic neuropathy.Eur J Ophthalmol. 2004 May-Jun;14(3):245-57. doi: 10.1177/112067210401400310. Eur J Ophthalmol. 2004. PMID: 15206651
-
Population-Based Performance of Inflammatory Markers in Giant Cell Arteritis.Am J Ophthalmol. 2025 Jul;275:47-51. doi: 10.1016/j.ajo.2025.03.022. Epub 2025 Mar 24. Am J Ophthalmol. 2025. PMID: 40139650
-
Temporal Artery Biopsy in the Workup of Giant Cell Arteritis: Diagnostic Considerations in a Veterans Administration Cohort.J Neuroophthalmol. 2020 Dec;40(4):450-456. doi: 10.1097/WNO.0000000000001040. J Neuroophthalmol. 2020. PMID: 32868573
-
Circulating CD8+ T cells in polymyalgia rheumatica and giant cell arteritis: a review.Semin Arthritis Rheum. 2001 Feb;30(4):257-71. doi: 10.1053/sarh.2001.9734. Semin Arthritis Rheum. 2001. PMID: 11182026 Review.
-
Significance of inflammation restricted to adventitial/periadventitial tissue on temporal artery biopsy.Semin Arthritis Rheum. 2020 Oct;50(5):1064-1072. doi: 10.1016/j.semarthrit.2020.05.021. Epub 2020 Jun 17. Semin Arthritis Rheum. 2020. PMID: 32911285 Review.
Cited by
-
[Laboratory diagnostics for vasculitis beyond antineutrophil cytoplasmatic autoantibodies].Z Rheumatol. 2024 May;83(4):283-296. doi: 10.1007/s00393-024-01494-y. Epub 2024 Apr 8. Z Rheumatol. 2024. PMID: 38587633 Review. German.
-
Normal ESR, CRP and Platelet Count in Giant Cell Arteritis and Polymyalgia Rheumatica: A Diagnostic Conundrum.Eur J Case Rep Intern Med. 2022 Feb 21;9(2):003192. doi: 10.12890/2022_003192. eCollection 2022. Eur J Case Rep Intern Med. 2022. PMID: 35265557 Free PMC article.
-
Aptamers for Proteins Associated with Rheumatic Diseases: Progress, Challenges, and Prospects of Diagnostic and Therapeutic Applications.Biomedicines. 2020 Nov 22;8(11):527. doi: 10.3390/biomedicines8110527. Biomedicines. 2020. PMID: 33266394 Free PMC article. Review.
-
Causal genes identification of giant cell arteritis in CD4+ Memory t cells: an integration of multi-omics and expression quantitative trait locus analysis.Inflamm Res. 2025 Jan 7;74(1):3. doi: 10.1007/s00011-024-01965-7. Inflamm Res. 2025. PMID: 39762453 Free PMC article.
-
Risk Factors and Pharmacological Interventions Impacting Cerebrovascular Ischemic Events in Giant Cell Arteritis: A Narrative Review.Immun Inflamm Dis. 2025 Jan;13(1):e70122. doi: 10.1002/iid3.70122. Immun Inflamm Dis. 2025. PMID: 39817601 Free PMC article. Review.
References
-
- Horton BT, Magath TB, Brown GE. An undescribed form of arteritis of the temporal vessels. Proc Staff Meet Mayo Clin. 1932;7:700–701.
-
- Lie JT. Temporal artery biopsy diagnosis of giant cell arteritis: lessons from 1109 biopsies. Anat Pathol. 1996;1:69–97. - PubMed
-
- Hellmann DB. Giant cell arteritis and polymyalgia rheumatica. In: Imboden JB, Hellmann DB, S JH, editors. Current rheumatology diagnosis and treatment. New York: McGraw Hill; 2004. pp. 235–241.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
