

Estimating outcome probabilities from early symptom changes in cognitive therapy for recurrent depression
- PMID: 31008632
- PMCID: PMC6853186
- DOI: 10.1037/ccp0000409
Estimating outcome probabilities from early symptom changes in cognitive therapy for recurrent depression
Abstract
Objective: Acute-phase cognitive therapy (CT) is an efficacious treatment for major depressive disorder (MDD) producing benefits comparable to pharmacotherapy, but not all patients respond or remit. The purpose of the current analyses was to estimate CT patients' probability of nonresponse and remission from symptom improvement early in treatment.
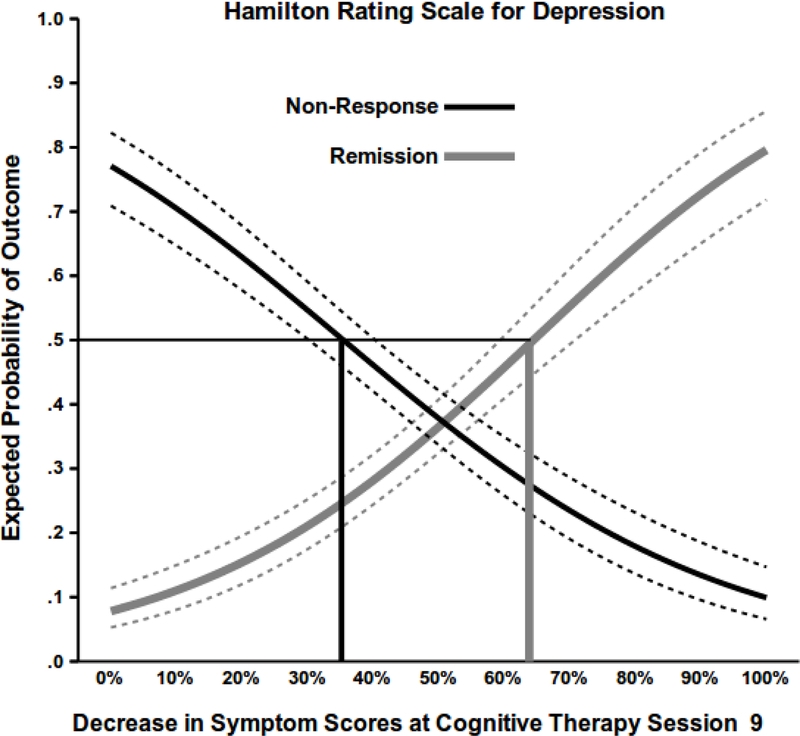
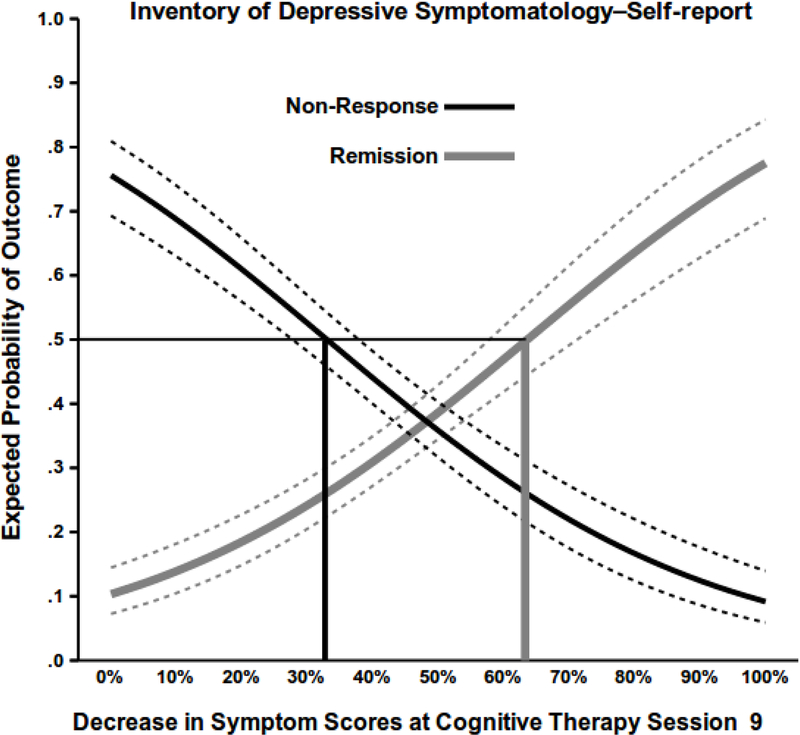
Method: Data from 2 clinical trials of acute-phase CT for recurrent depression were pooled for analysis (N = 679). Adult outpatients received 16- or 20-session CT protocols. Symptoms were measured repeatedly with the clinician-report Hamilton Rating Scale for Depression (HRSD) and Inventory of Depressive Symptomatology-Self-Report (IDS-SR). Outcomes at exit from CT were nonresponse (<50% reduction in HRSD scores) and remission (no MDD and HRSD score ≤6).
Results: The nonresponse rate was 45.7%, and the remission rate was 33.4%. In logistic regression models, improvements on the HRSD or IDS-SR from intake to CT Sessions 3, 5, 7, 9, or 11 significantly predicted both outcomes, with prediction gaining in accuracy in later sessions. Clinician and self-report assessments yielded similar results. Prediction of outcomes replicated across data sets. Patients with no symptom improvement by CT Session 9 (Week 5) had ≤10% probability of remission and >75% probability of nonresponse.
Conclusions: Outcomes of CT for depression are predictable from early symptom changes. Clinicians may find nonresponse and remission probability estimates useful in the informed consent process and in choosing whether to continue, augment, or switch treatments for CT patients with recurrent MDD. (PsycINFO Database Record (c) 2019 APA, all rights reserved).
Figures
References
-
- Aderka IM, Nickerson A, Bøe HJ, & Hofmann SG (2012). Sudden gains during psychological treatments of anxiety and depression: A meta-analysis. Journal of Consulting and Clinical Psychology, 80, 93–101. - PubMed
-
- American Psychiatric Association. (1994). Diagnostic and Statistical Manual of Mental Disorders (4th ed.). Washington, DC: Author.
-
- American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.). Washington, DC: Author.
-
- Barkham M, Connell J, Stiles WB, Miles JNV, Margison F, Evans C, & Mellor-Clark J. (2006). Dose-effect relations and responsive regulation of treatment duration: the good enough level. Journal of Consulting and Clinical Psychology, 74, 160–167. - PubMed
-
- Beck AT, & Haigh EP (2014). Advances in cognitive theory and therapy: The generic cognitive model. Annual Review of Clinical Psychology, 10, 1–24. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
