

Small Intestinal Bacterial Overgrowth Is Common in Chronic Pancreatitis and Associates With Diabetes, Chronic Pancreatitis Severity, Low Zinc Levels, and Opiate Use
- PMID: 31008737
- PMCID: PMC6610753
- DOI: 10.14309/ajg.0000000000000200
Small Intestinal Bacterial Overgrowth Is Common in Chronic Pancreatitis and Associates With Diabetes, Chronic Pancreatitis Severity, Low Zinc Levels, and Opiate Use
Abstract
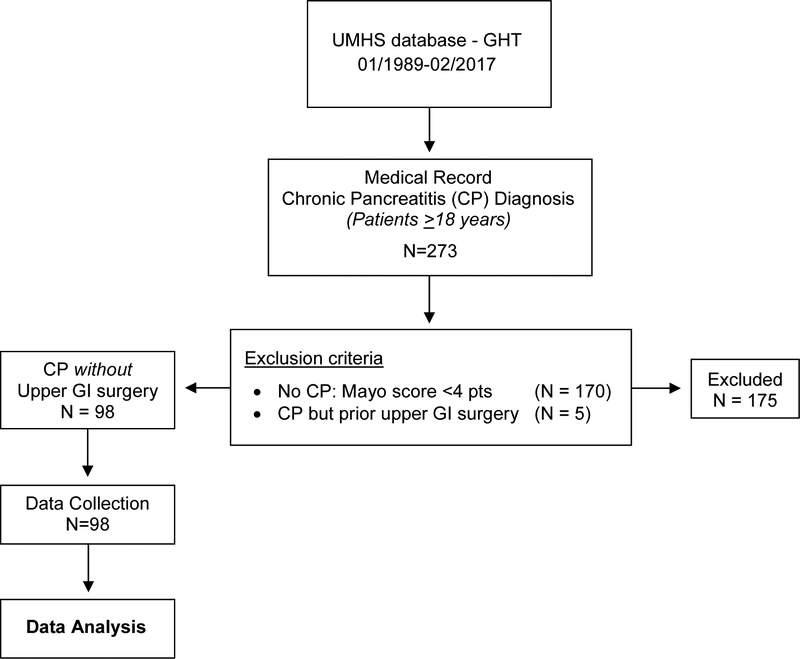
Objectives: Small intestinal bacterial overgrowth (SIBO) is often present in patients with chronic pancreatitis (CP) with persistent steatorrhea, despite pancreatic enzyme replacement therapy. Overall prevalence of SIBO, diagnosed by glucose breath test (GBT), varies between 0% and 40% but 0%-21% in those without upper gastrointestinal (GI) surgery. We investigated the prevalence and nonsurgical independent predictors of SIBO in CP without upper GI surgery.
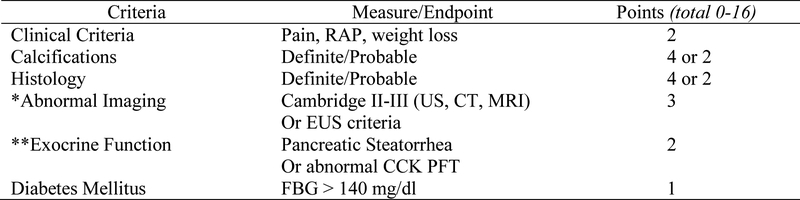
Methods: Two hundred seventy-three patients ≥18 years old had a presumptive diagnosis of CP and a GBT between 1989 and 2017. We defined CP by Mayo score (0-16) ≥4 and a positive GBT for SIBO by Rome consensus criteria and retrospectively collected data for 5 a priori variables (age, opiates, alcohol use, diabetes mellitus (DM), gastroparesis) and 41 investigational variables (demographics, GI symptoms, comorbidities, CP etiologies and cofactors, CP symptom duration, Mayo score and nondiabetes components, and biochemical variables).
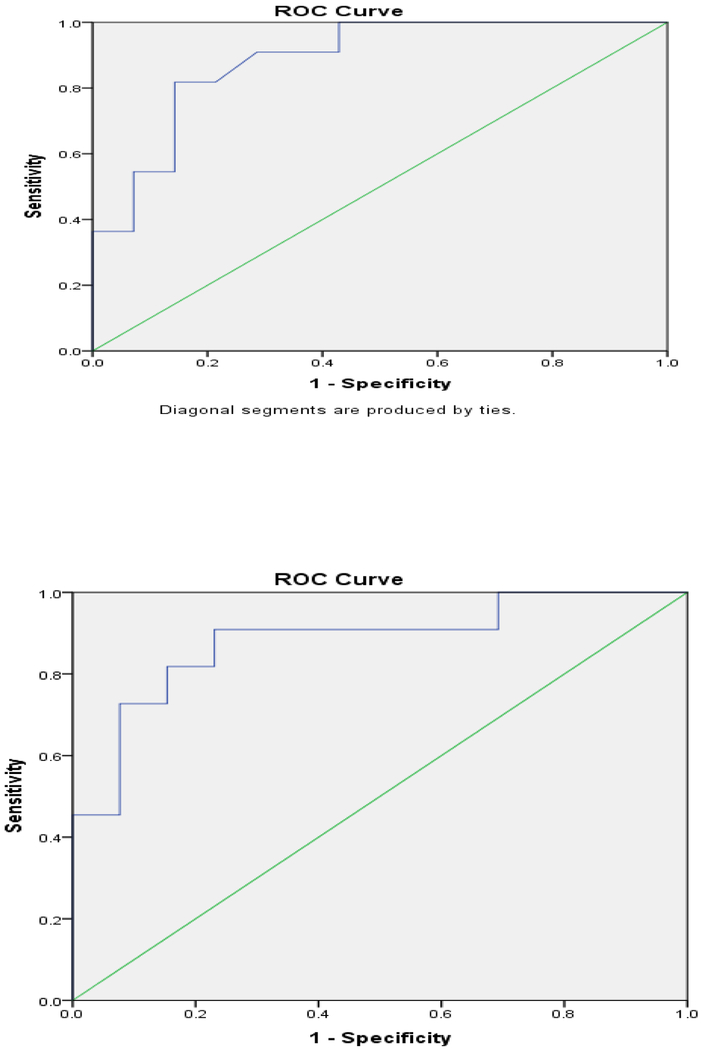
Results: Ninety-eight of 273 patients had definite CP and 40.8% had SIBO. Five of 46 variables predicted SIBO: opiates, P = 0.005; DM, P = 0.04; total Mayo score, P < 0.05; zinc, P = 0.005; and albumin, P < 0.05). Multivariable analysis of 3 noncorrelated variables identified zinc level (odds ratio = 0.0001; P = 0.03) as the sole independent predictor of SIBO (model C-statistic = 0.89; P < 0.001).
Discussion: SIBO, diagnosed by GBT, occurs in 40.8% of patients with CP without upper GI surgery. In patients with CP, markers of more severe CP (low zinc level, DM and increased Mayo score) and opiate use should raise clinical suspicion for SIBO, particularly in patients with persistent steatorrhea or weight loss despite pancreatic enzyme replacement therapy.
Conflict of interest statement
Potential competing interests: No authors declare competing interests (AAL, EJW, JRB, MJD, RS).
Figures
Similar articles
-
The prevalence of small intestinal bacterial overgrowth in non-surgical patients with chronic pancreatitis and pancreatic exocrine insufficiency (PEI).Pancreatology. 2018 Jun;18(4):379-385. doi: 10.1016/j.pan.2018.02.010. Epub 2018 Feb 24. Pancreatology. 2018. PMID: 29502987
-
Small intestinal bacterial overgrowth in patients with chronic pancreatitis.J Clin Gastroenterol. 2014 Nov-Dec;48 Suppl 1:S52-5. doi: 10.1097/MCG.0000000000000238. J Clin Gastroenterol. 2014. PMID: 25291129
-
Small intestinal bacterial overgrowth is common both among patients with alcoholic and idiopathic chronic pancreatitis.Pancreatology. 2014 Jul-Aug;14(4):280-3. doi: 10.1016/j.pan.2014.05.792. Epub 2014 May 27. Pancreatology. 2014. PMID: 25062877
-
Factors That Affect Prevalence of Small Intestinal Bacterial Overgrowth in Chronic Pancreatitis: A Systematic Review, Meta-Analysis, and Meta-Regression.Clin Transl Gastroenterol. 2019 Sep;10(9):e00072. doi: 10.14309/ctg.0000000000000072. Clin Transl Gastroenterol. 2019. PMID: 31517648 Free PMC article.
-
Small Intestinal Bacterial Overgrowth in Functional Dyspepsia: A Systematic Review and Meta-Analysis.Am J Gastroenterol. 2021 May 1;116(5):935-942. doi: 10.14309/ajg.0000000000001197. Am J Gastroenterol. 2021. PMID: 33734110
Cited by
-
Exocrine Pancreatic Dysfunction Increases the Risk of New-Onset Diabetes Mellitus: Results of a Nationwide Cohort Study.Clin Transl Sci. 2021 Jan;14(1):170-178. doi: 10.1111/cts.12837. Epub 2020 Jul 21. Clin Transl Sci. 2021. PMID: 32692901 Free PMC article.
-
Gut Microbiota as a Mediator of Essential and Toxic Effects of Zinc in the Intestines and Other Tissues.Int J Mol Sci. 2021 Dec 3;22(23):13074. doi: 10.3390/ijms222313074. Int J Mol Sci. 2021. PMID: 34884881 Free PMC article. Review.
-
New Insights into Chronic Pancreatitis: Potential Mechanisms Related to Probiotics.Microorganisms. 2024 Aug 24;12(9):1760. doi: 10.3390/microorganisms12091760. Microorganisms. 2024. PMID: 39338435 Free PMC article. Review.
-
The Influence of Small Intestinal Bacterial Overgrowth in Digestive and Extra-Intestinal Disorders.Int J Mol Sci. 2020 May 16;21(10):3531. doi: 10.3390/ijms21103531. Int J Mol Sci. 2020. PMID: 32429454 Free PMC article. Review.
-
Mucosa-Associated Microbial Profile Is Altered in Small Intestinal Bacterial Overgrowth.Front Microbiol. 2021 Jul 30;12:710940. doi: 10.3389/fmicb.2021.710940. eCollection 2021. Front Microbiol. 2021. PMID: 34421869 Free PMC article.
References
-
- Forsmark CE: Management of chronic pancreatitis. Gastroenterology 2013, 144:1282–1291e1283. - PubMed
-
- DiMagno MJ, Wamsteker EJ, Lee A: Chronic Pancreatitis. In BMJ Point-of-Care 2018. Edited by. www.pointofcare.bmj.com (Last accessed November 17, 2017); 2017.
-
- Mullady DK, Yadav D, Amann ST, O’Connell MR, Barmada MM, Elta GH, Scheiman JM, Wamsteker EJ, Chey WD, Korneffel ML, et al.: Type of pain, pain-associated complications, quality of life, disability and resource utilisation in chronic pancreatitis: a prospective cohort study. Gut 2011, 60:77–84. - PMC - PubMed
-
- Wehler M, Nichterlein R, Fischer B, Farnbacher M, Reulbach U, Hahn EG, Schneider T: Factors associated with health-related quality of life in chronic pancreatitis. Am J Gastroenterol 2004, 99:138–146. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
