

The efficacy of renal replacement therapy strategies for septic-acute kidney injury: A PRISMA-compliant network meta-analysis
- PMID: 31008965
- PMCID: PMC6494389
- DOI: 10.1097/MD.0000000000015257
The efficacy of renal replacement therapy strategies for septic-acute kidney injury: A PRISMA-compliant network meta-analysis
Abstract
Background: Renal replacement therapy (RRT) is the main treatment for patients with sepsis-induced acute kidney injury (SAKI). However, the choice of RRT strategy remains controversial.
Objective: This study assessed the effectiveness of RRT variants in SAKI patients by a network meta-analysis.
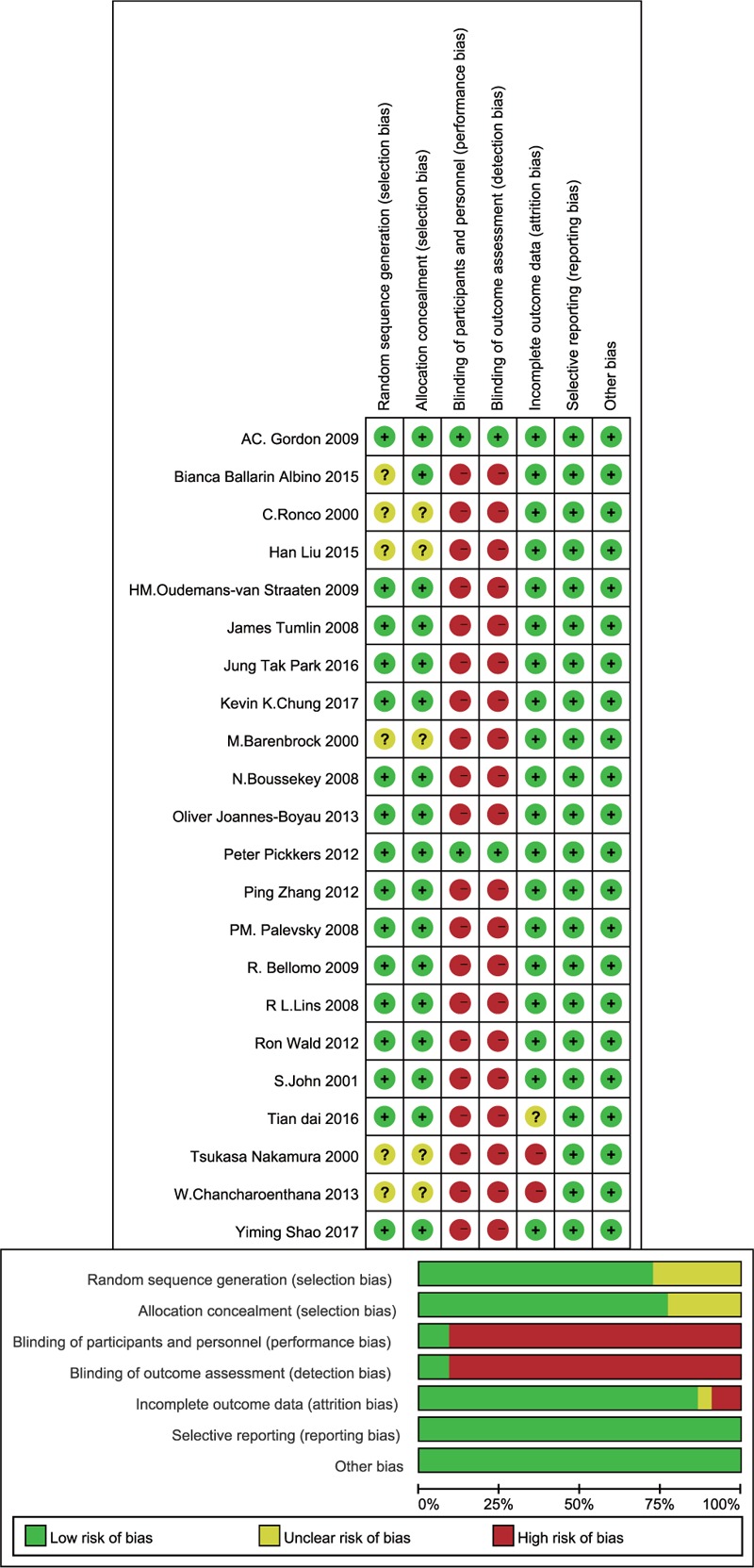
Methods: This study searched the literature in the PubMed, EmBase, and Cochrane Library databases up to August 18, 2018. The outcomes of the analysis were the survival rate, renal recovery rate, intensive care unit (ICU) duration, and hospital duration.
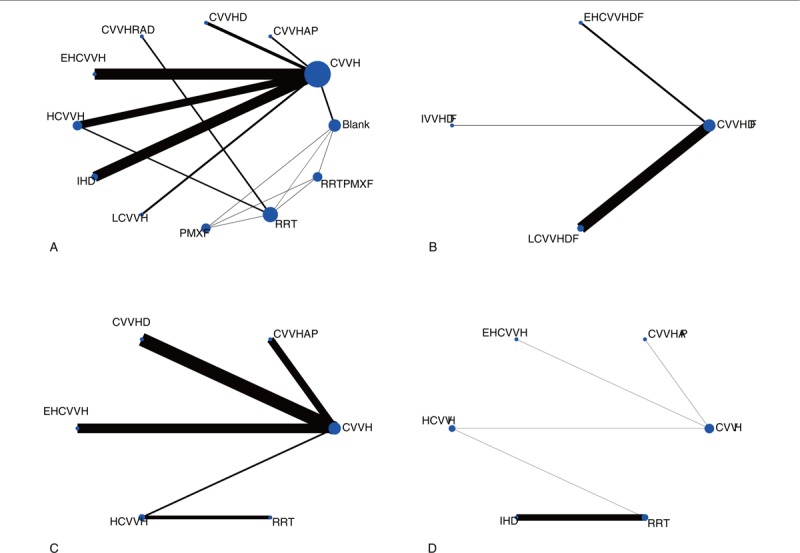
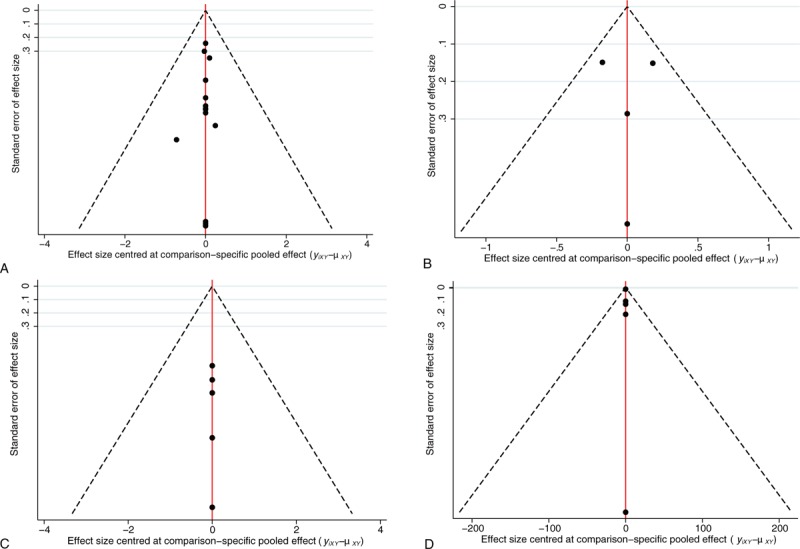
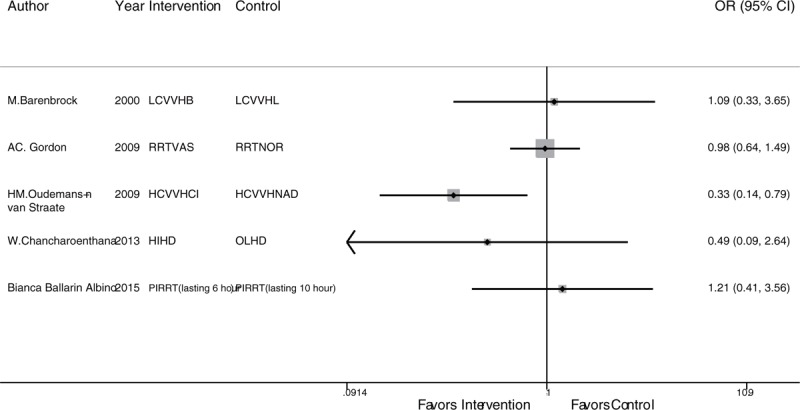
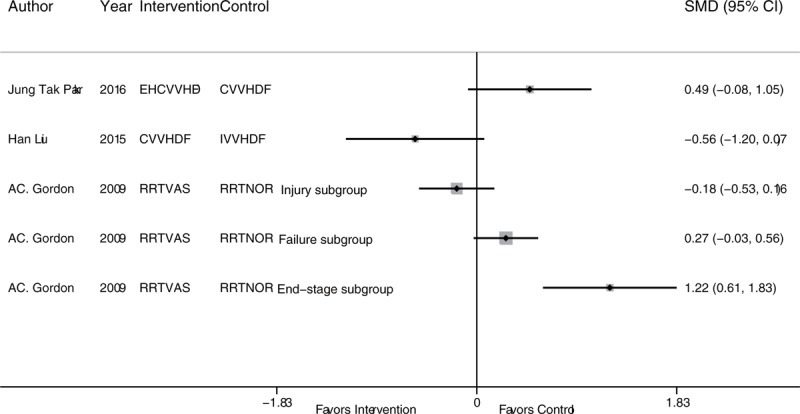
Results: Twenty-two articles were included in the analysis. The results showed that only the negative control was inferior to the regimens of RRT with polymyxin B-immobilized fiber (PMXF), PMXF alone, continuous venovenous hemofiltration (CVVH), CVVH plus alkaline phosphatase (AP), continuous venovenous hemodialysis (CVVHD), high-volume CVVH, and extra high-volume CVVH in terms of the survival rate. According to the surface under the cumulative ranking , RRT with PMXF (84.4%) and PMXF (84.3%) were the treatments most likely to improve the survival rate among SAKI patients, followed by CVVH plus AP (69%). Continuous venovenous hemodiafiltration (CVVHDF), extra high-volume CVVHDF, intermittent venovenous hemodiafiltration (IVVHDF), and low-volume CVVHDF resulted in very similar survival rates. CVVH plus AP conferred relative advantages in the renal recovery rate and ICU duration.
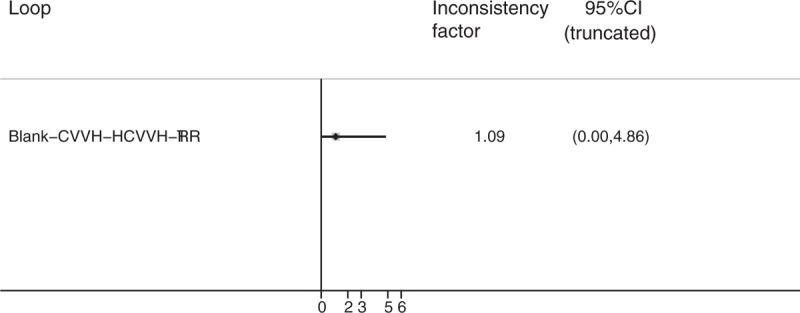
Conclusion: CVVH, CVVHD, and their derived RRT strategies can improve survival rates in SAKI patients, but there is no significant difference among the RRT strategies. There was also no significant difference in the survival rate among CVVHDF, IVVHDF, and their derived strategies. More high-quality randomized controlled trials with large sample sizes are needed for further research.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
