

Severity stratification and prognostic prediction of patients with acute pancreatitis at early phase: A retrospective study
- PMID: 31008971
- PMCID: PMC6494233
- DOI: 10.1097/MD.0000000000015275
Severity stratification and prognostic prediction of patients with acute pancreatitis at early phase: A retrospective study
Abstract
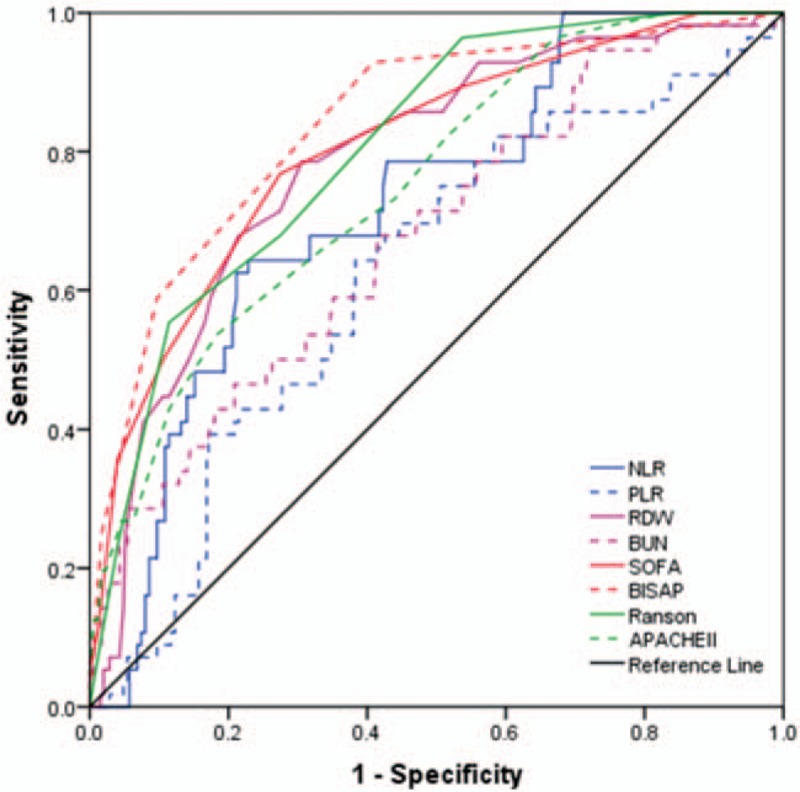
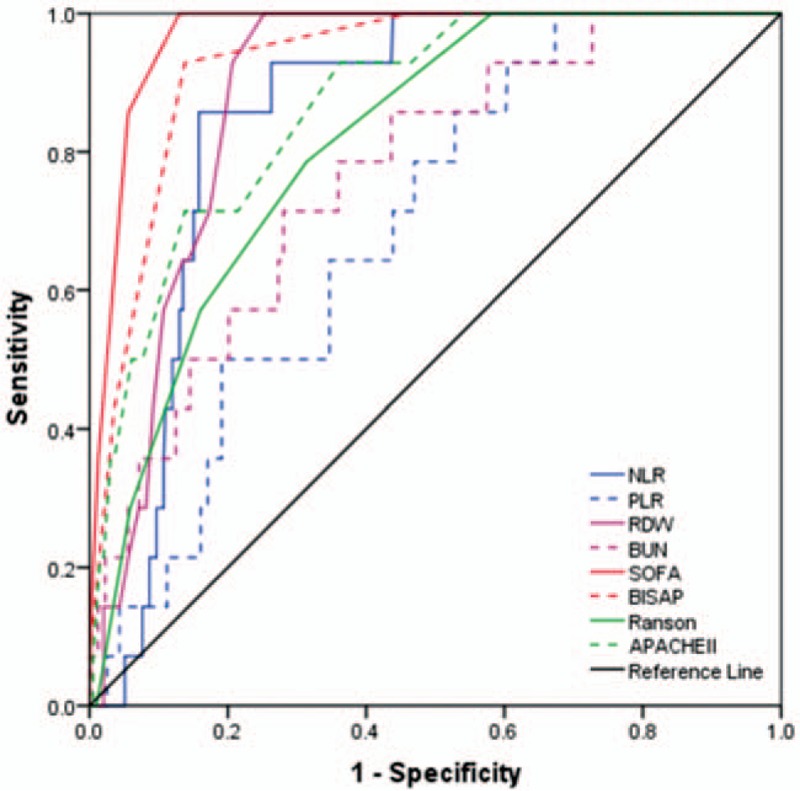
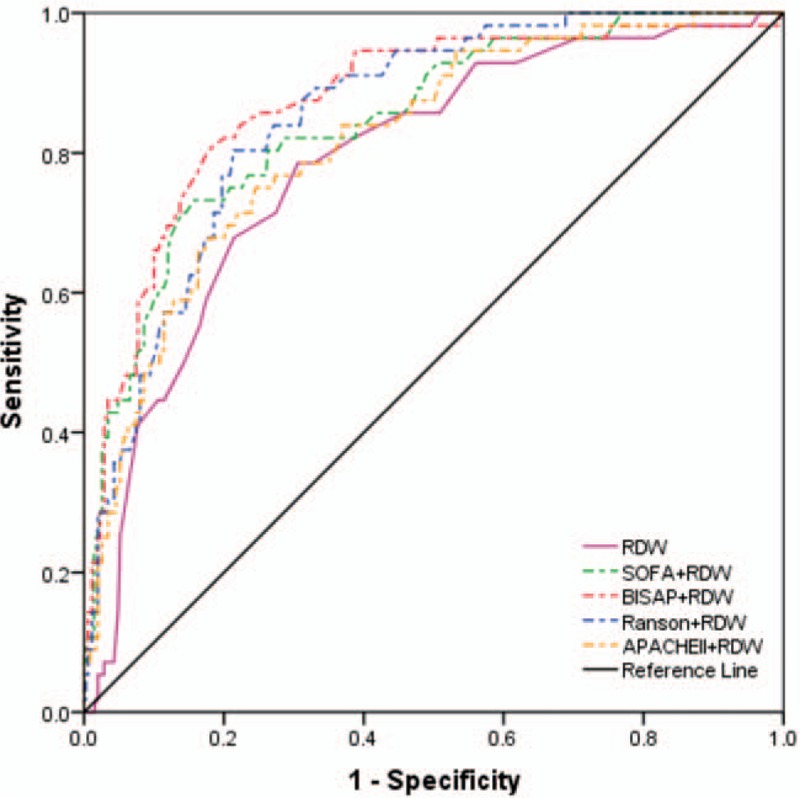
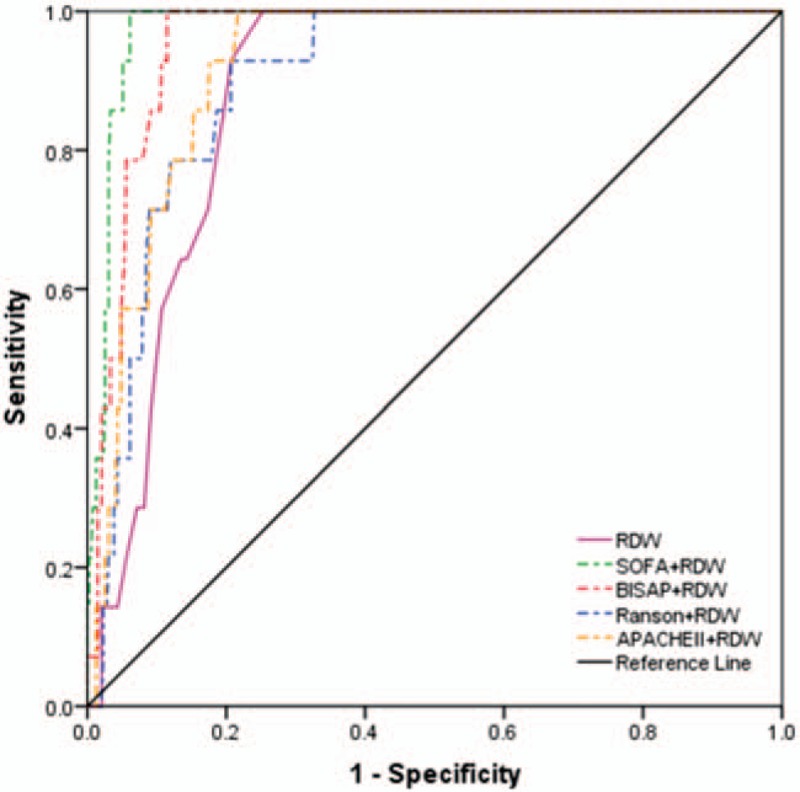
Severity stratification and prognostic prediction at early stage is crucial for reducing the rates of mortality of patients with acute pancreatitis (AP). We aim to investigate the predicting performance of neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR), and red-cell distribution width (RDW) combined with severity scores (sequential organ failure assessment [SOFA], bed-side index for severity of AP [BISAP], Ranson criteria, and acute physiology and chronic health evaluation II [APACHE II]) for severe AP (SAP) and mortality.A total of 406 patients diagnosed with AP admitted in a tertiary teaching hospital were enrolled. Demographic information and clinical parameters were retrospectively collected and analyzed. NLR, PLR, RDW, blood urea nitrogen (BUN), and AP severity scores (SOFA, BISAP, Ranson, and APACHE II) were compared between different severity groups and the survival and death group. Receiver-operating characteristic (ROC) curves for SAP and 28-day mortality were calculated for each predictor using cut-off values. Area under the curve (AUC) analysis and logistic regression models were performed to compare the performance of laboratory biomarkers and severity scores.Our results showed that NLR, PLR, RDW, glucose, and BUN level of the SAP group were significantly increased compared to the mild acute pancreatitis (MAP) group on admission (P < .001). The severity of AP increased as the NLR, SOFA, BISAP, and Ranson increased (P < .01). The AUC values of NLR, PLR, RDW, BUN, SOFA, BISAP, Ranson, and APACHE II to predict SAP were 0.722, 0.621, 0.787, 0.677, 0.806, 0.841, 0.806, and 0.752, respectively, while their AUC values to predict 28-day mortality were 0.851, 0.693, 0.885, 0.765, 0.968, 0.929, 0.812, and 0.867, respectively. BISAP achieved the highest AUC, sensitivity and NPV in predicting SAP, while SOFA is the most superior in predicting mortality. The combination of BISAP + RDW achieved the highest AUC (0.872) in predicting SAP and the combination of SOFA + RDW achieved the highest AUC (0.976) in predicting mortality. RDW (OR = 1.739), SOFA (OR = 1.554), BISAP (OR = 2.145), and Ranson (OR = 1.434) were all independent risk factors for predicting SAP, while RDW (OR = 7.361) and hematocrit (OR = 0.329) were independent risk factors for predicting mortality by logistic regression model.NLR, PLR, RDW, and BUN indicated good predictive value for SAP and mortality, while RDW had the highest discriminatory capacity. RDW is a convenient and reliable indicator for prediction not only SAP, but also mortality.
Figures
References
-
- Tenner S, Baillie J, DeWitt J, et al. American College of Gastroenterology guideline: management of acute pancreatitis. Am J Gastroenterol 2013;108:1400–15. 1416. - PubMed
-
- Renner IG, Savage WT, 3rd, Pantoja JL, et al. Death due to acute pancreatitis. A retrospective analysis of 405 autopsy cases. Dig Dis Sci 1985;30:1005–18. - PubMed
-
- Gloor B, Müller CA, Worni M, et al. Late mortality in patients with severe acute pancreatitis. Br J Surg 2001;88:975–9. - PubMed
-
- Juneja D, Gopal PB, Ravula M. Scoring systems in acute pancreatitis: which one to use in intensive care units? J Crit Care 2010;25:358.e9–15. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
