

Schizoaffective disorder comorbid with type 2 diabetes mellitus accompanied by frontotemporal atrophy and impaired cognition: A CARE compliant case report
- PMID: 31008977
- PMCID: PMC6494280
- DOI: 10.1097/MD.0000000000015292
Schizoaffective disorder comorbid with type 2 diabetes mellitus accompanied by frontotemporal atrophy and impaired cognition: A CARE compliant case report
Abstract
Rationale: Brain atrophy coupled with impaired cognition may be a sign of dementia. However, growing evidence indicates that schizoaffective disorder (SAD) and type 2 diabetes mellitus (T2DM) play roles in the processes of frontotemporal atrophy and cognitive decline. Few cases of frontotemporal atrophy and impaired cognition have been reported in young adult patients with SAD and T2DM.
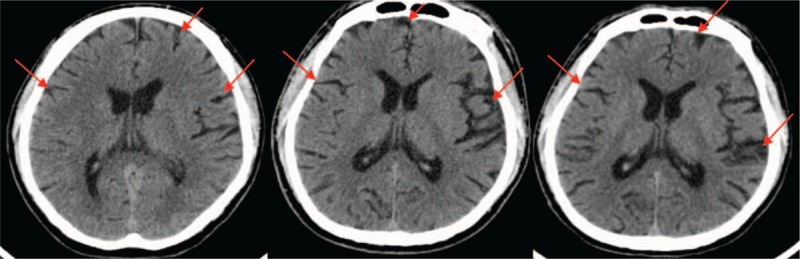
Patient concerns: A 34-year-old man was admitted for his 19th rehospitalization due to auditory verbal hallucinations (AVHs), delusions of persecution, mania, and fluctuating blood sugar levels. After admission, a brain computed tomography (CT) scan revealed that the patient's frontotemporal atrophy, which was first found in 2014, had gradually degenerated over time. The Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) revealed cognitive impairments. Based on the clinical assessment, his cognition and social function impairments were determined to mainly result from SAD and T2DM because the clinical characteristics and course of the disease did not coincide with the features of progressive aggravation of dementia.
Diagnoses: Diagnoses include the following: SAD-mania and T2DM.
Interventions: Paliperidone and sodium valproate coupled with quetiapine add-on treatment were prescribed for the patient.
Outcomes: The therapeutic strategy had a limited effect on the patient.
Lessons: Early onset of SAD and T2DM, as well as irregular treatment, resulting in brain atrophy coupled with cognitive impairments, may be the main causes of the patient's treatment resistance and poor outcome. The risks and benefits of treatment strategies should be individually assessed. Further neuroimaging, pertinent biomarkers, and genetic tests along with long-term follow-up are needed for precise evaluation of the patient's condition.
Conflict of interest statement
The authors have no conflicts of interest to declare with respect to the manuscript, with no financial, consultant, political, personal, religious, ideological, academic, intellectual, or other relationships that could lead to a conflict of interest.
Figures
Similar articles
-
[Frontal dementia or dementia praecox? A case report of a psychotic disorder with a severe decline].Encephale. 2003 Mar-Apr;29(2):172-80. Encephale. 2003. PMID: 14567169 French.
-
Brain imaging correlates of mild cognitive impairment and early dementia in patients with type 2 diabetes mellitus.Nutr Metab Cardiovasc Dis. 2018 Dec;28(12):1253-1260. doi: 10.1016/j.numecd.2018.07.008. Epub 2018 Aug 2. Nutr Metab Cardiovasc Dis. 2018. PMID: 30355471
-
Type 2 diabetes mellitus, brain atrophy and cognitive decline in older people: a longitudinal study.Diabetologia. 2019 Mar;62(3):448-458. doi: 10.1007/s00125-018-4778-9. Epub 2018 Dec 13. Diabetologia. 2019. PMID: 30547230
-
Frontotemporal Dysfunction and Dementia in Amyotrophic Lateral Sclerosis.Neurol Clin. 2015 Nov;33(4):787-805. doi: 10.1016/j.ncl.2015.07.011. Epub 2015 Sep 8. Neurol Clin. 2015. PMID: 26515622 Review.
-
Major depressive disorder with psychotic features may lead to misdiagnosis of dementia: a case report and review of the literature.J Psychiatr Pract. 2011 Nov;17(6):432-8. doi: 10.1097/01.pra.0000407968.57475.ab. J Psychiatr Pract. 2011. PMID: 22108402 Free PMC article. Review.
References
-
- Folstein MF, Folstein SE, McHugh PR. “Mini-mental state.” A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189–98. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
