

Dose Dependency of Iatrogenic Glucocorticoid Excess and Adrenal Insufficiency and Mortality: A Cohort Study in England
- PMID: 31009052
- PMCID: PMC6656418
- DOI: 10.1210/jc.2019-00153
Dose Dependency of Iatrogenic Glucocorticoid Excess and Adrenal Insufficiency and Mortality: A Cohort Study in England
Abstract
Context: Adrenal insufficiency and Cushing syndrome are known adverse events of glucocorticoids. However, no population estimates of dose-related risks are available.
Objective: To investigate dose-related risks of adrenal dysfunction and death in adults with six chronic inflammatory diseases treated with oral glucocorticoids.
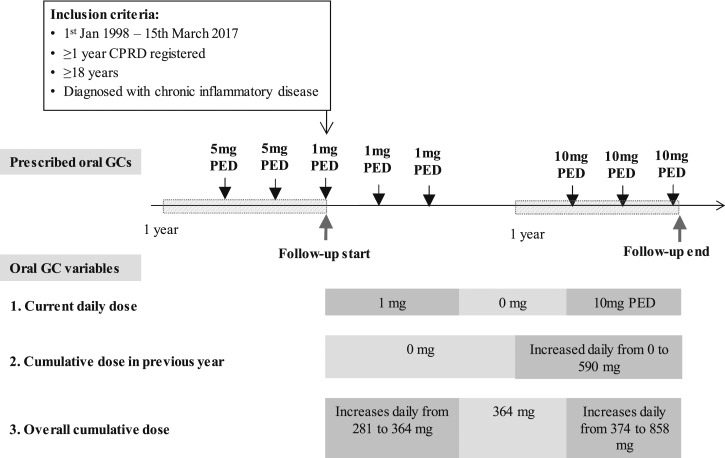
Design and setting: Retrospective, record-linkage, open-cohort study spanning primary and hospital care in England.
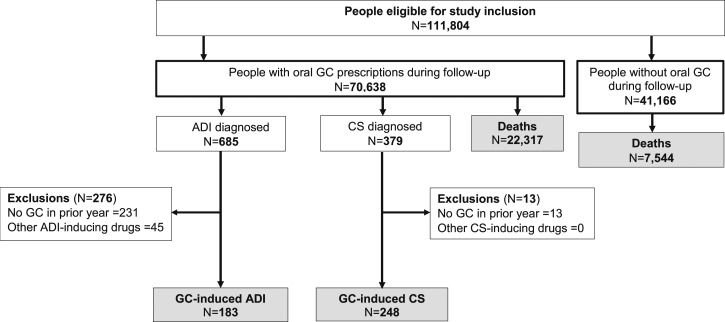
Patients: A total of 70,638 oral glucocorticoid users and 41,166 nonusers aged ≥18 years registered in 389 practices in 1998 to 2017.
Main outcome measures: Incidence rates and hazard ratios (HRs) of diagnosed adrenal dysfunction and death.
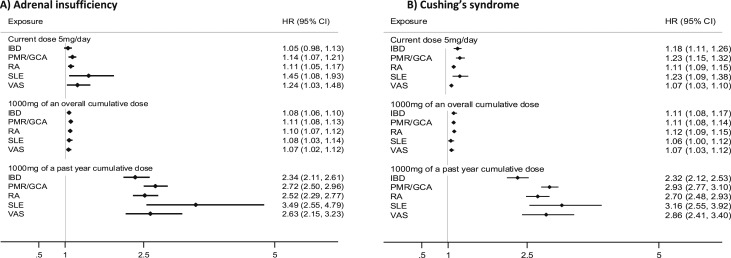
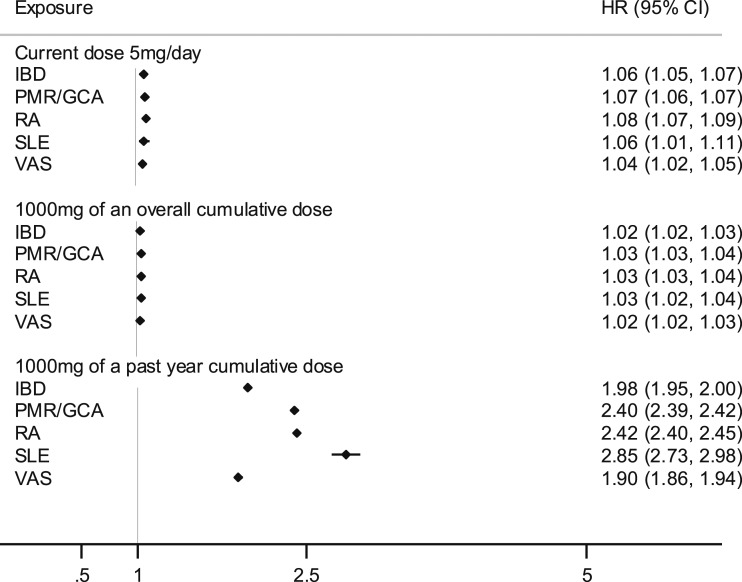
Results: During a median follow-up of 5.5 years, 183 patients had glucocorticoid-induced adrenal insufficiency and 248 had glucocorticoid-induced Cushing syndrome. A total of 22,317 (31.6%) and 7544 (18.3%) deaths occurred among glucocorticoid users and nonusers, respectively. The incidence of all outcomes increased with higher current daily and cumulative doses. For adrenal insufficiency, the increases in HRs were 1.07 (95% CI: 1.04 to 1.09) for every increase of 5 mg per day and 2.25 (95% CI: 2.15 to 2.35) per 1000 mg of cumulative prednisolone-equivalent dose over the past year. The respective increases in HRs for Cushing syndrome were 1.09 (95% CI: 1.08 to 1.11) and 2.31 (95% CI: 2.23 to 2.40) and for mortality 1.26 (95% CI: 2.24 to 1.28) and 2.05 (95% CI: 2.04 to 2.06).
Conclusion: We report a high glucocorticoid dose-dependent increased risk of adrenal adverse events and death. The low observed absolute risk of adrenal insufficiency highlights a potential lack of awareness and a need for increased physician and patient education about the risks of adrenal dysfunction induced by glucocorticoids.
Figures
References
-
- Broersen LH, Pereira AM, Jørgensen JO, Dekkers OM. Adrenal insufficiency in corticosteroids use: systematic review and meta-analysis. J Clin Endocrinol Metab. 2015;100(6):2171–2180. - PubMed
-
- Dixon WG, Bansback N. Understanding the side effects of glucocorticoid therapy: shining a light on a drug everyone thinks they know. Ann Rheum Dis. 2012;71(11):1761–1764. - PubMed
-
- Wei L, MacDonald TM, Walker BR. Taking glucocorticoids by prescription is associated with subsequent cardiovascular disease. Ann Intern Med. 2004;141(10):764–770. - PubMed
-
- Fardet L, Petersen I, Nazareth I. Prevalence of long-term oral glucocorticoid prescriptions in the UK over the past 20 years. Rheumatology (Oxford). 2011;50(11):1982–1990. - PubMed
-
- Newell-Price J, Bertagna X, Grossman AB, Nieman LK. Cushing’s syndrome. Lancet. 2006;367(9522):1605–1617. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
