

Prognostic performance of preoperative cardiac troponin and perioperative changes in cardiac troponin for the prediction of major adverse cardiac events and mortality in noncardiac surgery: A systematic review and meta-analysis
- PMID: 31009468
- PMCID: PMC6476502
- DOI: 10.1371/journal.pone.0215094
Prognostic performance of preoperative cardiac troponin and perioperative changes in cardiac troponin for the prediction of major adverse cardiac events and mortality in noncardiac surgery: A systematic review and meta-analysis
Abstract
Background: Increased postoperative cardiac troponin (cTn) independently predicts short-term mortality. Previous studies suggest that preoperative cTn also predicts major adverse cardiovascular events (MACE) and mortality after noncardiac surgery. The value of preoperative and perioperative changes in cTn as a prognostic tool for adverse outcomes has been sparsely investigated.
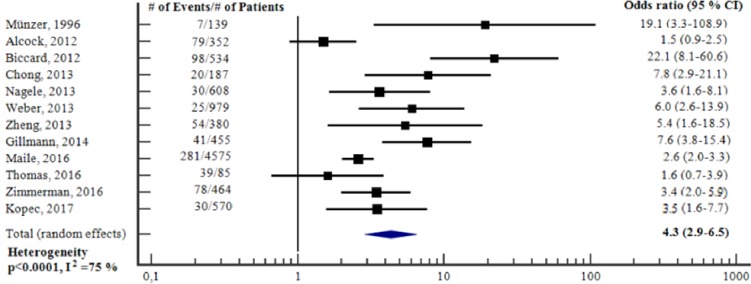
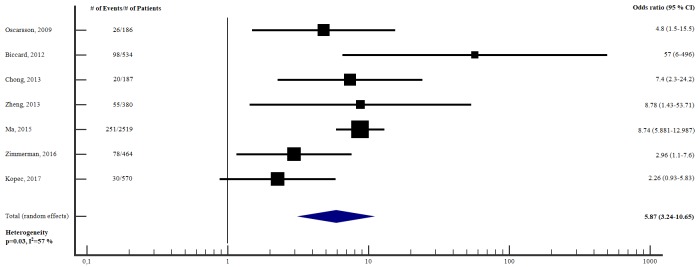
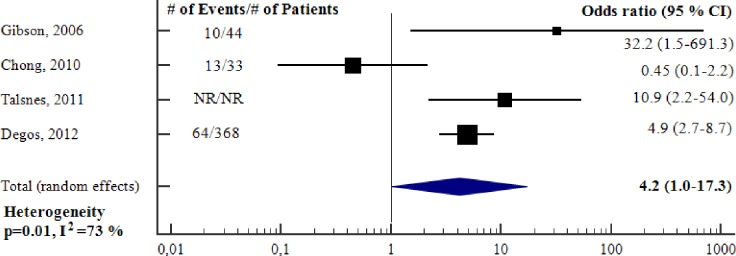
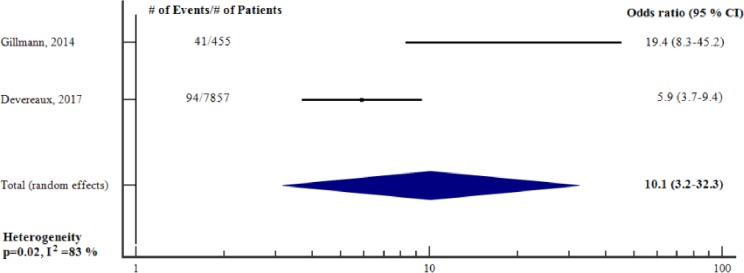
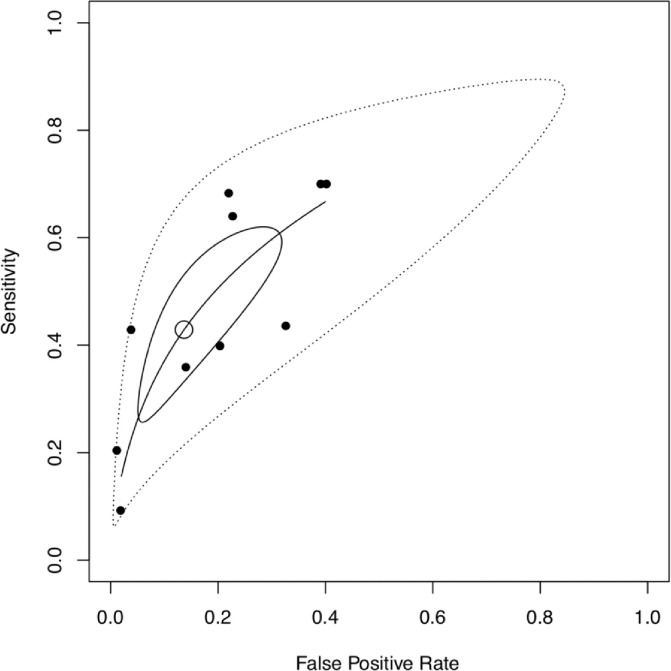
Methods and findings: A systematic review and meta-analysis of the prognostic value of cTns for adverse outcome was conducted. Adverse outcome was defined as short-term (in-hospital or <30 days) and long-term (>30 days) MACE and/or all-cause mortality, in adult patients undergoing noncardiac surgery. The study protocol (CRD42018094773) was registered with an international prospective register of systematic reviews (PROSPERO). Preoperative cTn was a predictor of short- (OR 4.3, 95% CI 2.9-6.5, p<0.001, adjusted OR 5.87, 95% CI 3.24-10.65, p<0.001) and long-term adverse outcome (OR 4.2, 95% CI 1.0-17.3, p = 0.05, adjusted HR 2.0, 95% CI 1.4-3.0, p<0.001). Perioperative change in cTn was a predictor of short-term adverse outcome (OR 10.1, 95% CI 3.2-32.3, p<0.001). It was not possible to conduct pooled analyses for adjusted estimates of perioperative change in cTn as predictor of short- (a single study identified) and long-term (no studies identified) adverse outcome. Further, it was not possible to conduct pooled analyses for unadjusted estimates of perioperative change in cTn as predictor of long-term adverse outcome, since only one study was identified. Bivariate analysis of sensitivities and specificities were performed, and overall prognostic performance was summarized using summary receiver operating characteristic (SROC) curves. The pooled sensitivity and specificity for preoperative cTn and short-term adverse outcome was 0.43 and 0.86 respectively (area under the SROC curve of 0.68). There were insufficient studies to construct SROCs for perioperative changes in cTn and for long-term adverse outcome.
Conclusion: Our study indicates that although preoperative cTn and perioperative change in cTn might be valuable predictors of MACE and/or all-cause mortality in adult noncardiac surgical patients, its overall prognostic performance remains uncertain. Future large, representative, high-quality studies are needed to establish the potential role of cTns in perioperative cardiac risk stratification.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
A preliminary report on the prognostic significance of preoperative brain natriuretic peptide and postoperative cardiac troponin in patients undergoing major vascular surgery.Anesth Analg. 2009 Apr;108(4):1069-75. doi: 10.1213/ane.0b013e318194f3e6. Anesth Analg. 2009. PMID: 19299763 Clinical Trial.
-
Association of pre-operative troponin levels with major adverse cardiac events and mortality after noncardiac surgery: A systematic review and meta-analysis.Eur J Anaesthesiol. 2018 Nov;35(11):815-824. doi: 10.1097/EJA.0000000000000868. Eur J Anaesthesiol. 2018. PMID: 30095548
-
Postoperative elevated cardiac troponin levels predict all-cause mortality and major adverse cardiovascular events following noncardiac surgery: A dose-response meta-analysis of prospective studies.J Clin Anesth. 2023 Nov;90:111229. doi: 10.1016/j.jclinane.2023.111229. Epub 2023 Aug 11. J Clin Anesth. 2023. PMID: 37573706 Review.
-
Prognostic value of high-sensitivity cardiac troponin for major adverse cardiovascular events in patients with diabetes: a systematic review and meta-analysis.PeerJ. 2023 Nov 13;11:e16376. doi: 10.7717/peerj.16376. eCollection 2023. PeerJ. 2023. PMID: 38025710 Free PMC article.
-
Prognostic value of preoperative cardiac troponin I in patients with non-ST-segment elevation acute coronary syndromes undergoing coronary artery bypass surgery.Chest. 2005 Nov;128(5):3526-36. doi: 10.1378/chest.128.5.3526. Chest. 2005. PMID: 16304309
Cited by
-
Validation of Perioperative Troponin Levels for Predicting Postoperative Mortality and Long-Term Survival in Patients Undergoing Surgery for Hepatobiliary and Pancreatic Cancer.J Cardiovasc Dev Dis. 2024 Apr 22;11(4):130. doi: 10.3390/jcdd11040130. J Cardiovasc Dev Dis. 2024. PMID: 38667748 Free PMC article.
-
Assessment of the prognostic value of preoperative high-sensitive troponin T for myocardial injury and long-term mortality for groups at high risk for cardiovascular events following noncardiac surgery: a retrospective cohort study.Front Med (Lausanne). 2023 Jun 22;10:1135786. doi: 10.3389/fmed.2023.1135786. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37425305 Free PMC article.
-
Prognostic value of high-sensitivity cardiac troponin in non-cardiac surgical patients in intensive care units.Intern Emerg Med. 2024 Jan;19(1):201-209. doi: 10.1007/s11739-023-03509-z. Epub 2024 Jan 9. Intern Emerg Med. 2024. PMID: 38194002 Free PMC article.
-
Assessment and Management of Ischaemic Heart Disease in Non-Cardiac Surgery.Heart Int. 2023 Dec 1;17(2):19-26. doi: 10.17925/HI.2023.17.2.19. eCollection 2023. Heart Int. 2023. PMID: 38419719 Free PMC article. Review.
-
[Preoperative evaluation of adult patients before elective, non-cardiothoracic surgery : A joint recommendation of the German Society for Anesthesiology and Intensive Care Medicine, the German Society for Surgery and the German Society for Internal Medicine].Anaesthesiologie. 2024 May;73(5):294-323. doi: 10.1007/s00101-024-01408-2. Epub 2024 May 3. Anaesthesiologie. 2024. PMID: 38700730 Free PMC article. Review. German.
References
-
- Botto F, Alonso-Coello P, Chan MT, Villar JC, Xavier D, Srinathan S, et al. Myocardial injury after noncardiac surgery: a large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology. 2014;120: 564–78. 10.1097/ALN.0000000000000113 - DOI - PubMed
-
- Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100: 1043–9. - PubMed
-
- Alonso-Coello P, Paniagua P, Mizera R, Devereaux PJ. Should physicians initiate beta-blocker therapy in patients undergoing non-cardiac surgery? Insights from the POISE trial. Pol Arch Med Wewn. 2008;118: 616–8. - PubMed
-
- Weiser TG, Haynes AB, Molina G, Lipsitz SR, Esquivel MM, Uribe-Leitz T, et al. Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet. 2015;385 Suppl 2:S11. - PubMed
