

Deep Learning Predicts Lung Cancer Treatment Response from Serial Medical Imaging
- PMID: 31010833
- PMCID: PMC6548658
- DOI: 10.1158/1078-0432.CCR-18-2495
Deep Learning Predicts Lung Cancer Treatment Response from Serial Medical Imaging
Abstract
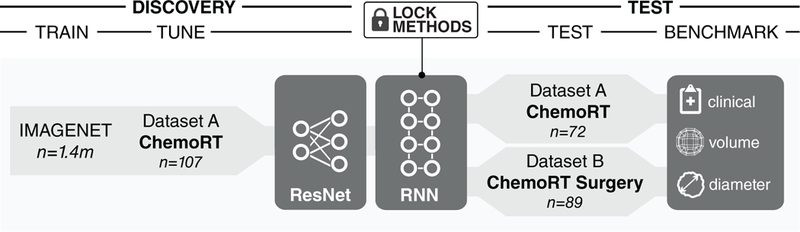
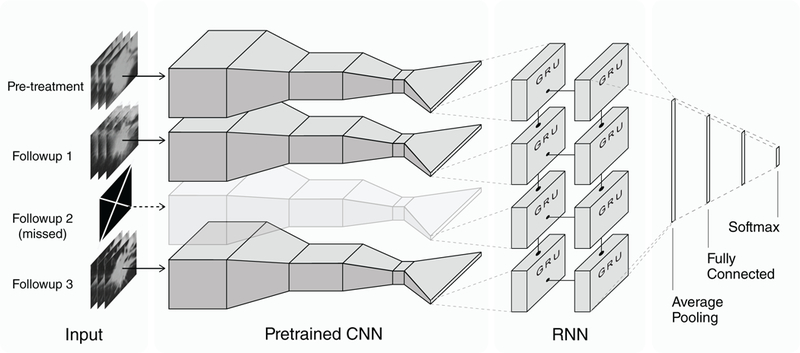
Purpose: Tumors are continuously evolving biological systems, and medical imaging is uniquely positioned to monitor changes throughout treatment. Although qualitatively tracking lesions over space and time may be trivial, the development of clinically relevant, automated radiomics methods that incorporate serial imaging data is far more challenging. In this study, we evaluated deep learning networks for predicting clinical outcomes through analyzing time series CT images of patients with locally advanced non-small cell lung cancer (NSCLC).Experimental Design: Dataset A consists of 179 patients with stage III NSCLC treated with definitive chemoradiation, with pretreatment and posttreatment CT images at 1, 3, and 6 months follow-up (581 scans). Models were developed using transfer learning of convolutional neural networks (CNN) with recurrent neural networks (RNN), using single seed-point tumor localization. Pathologic response validation was performed on dataset B, comprising 89 patients with NSCLC treated with chemoradiation and surgery (178 scans).
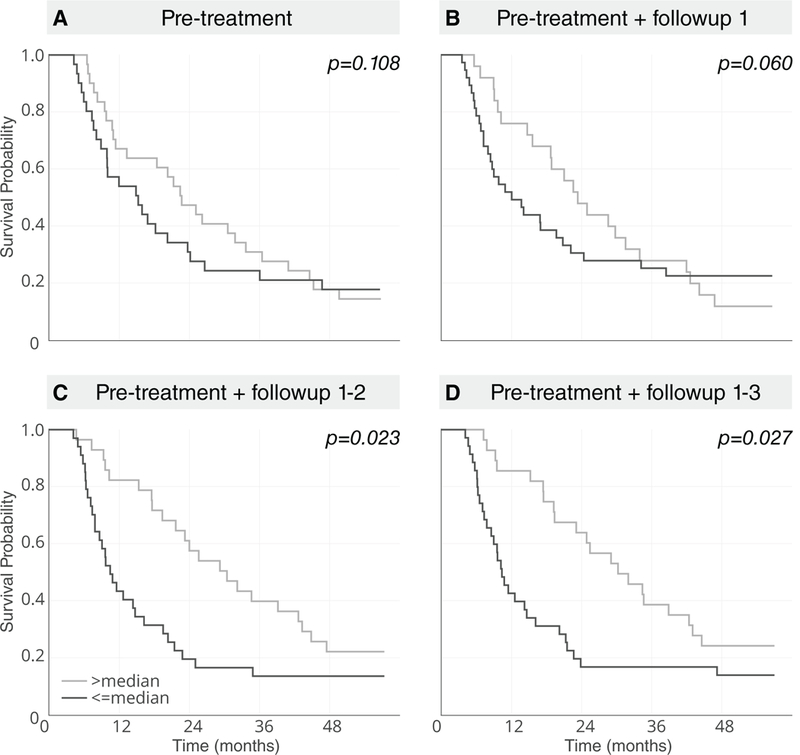
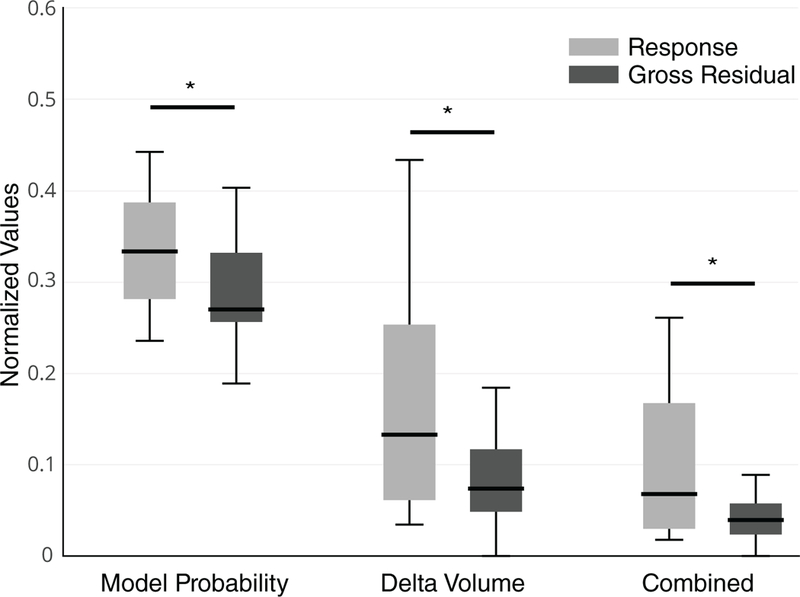
Results: Deep learning models using time series scans were significantly predictive of survival and cancer-specific outcomes (progression, distant metastases, and local-regional recurrence). Model performance was enhanced with each additional follow-up scan into the CNN model (e.g., 2-year overall survival: AUC = 0.74, P < 0.05). The models stratified patients into low and high mortality risk groups, which were significantly associated with overall survival [HR = 6.16; 95% confidence interval (CI), 2.17-17.44; P < 0.001]. The model also significantly predicted pathologic response in dataset B (P = 0.016).
Conclusions: We demonstrate that deep learning can integrate imaging scans at multiple timepoints to improve clinical outcome predictions. AI-based noninvasive radiomics biomarkers can have a significant impact in the clinic given their low cost and minimal requirements for human input.
©2019 American Association for Cancer Research.
Conflict of interest statement
Conflicts of Interests:
Hugo JWL Aerts reports shares from Genospace and Sphera, outside of submitted work.
Figures

References
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. - PubMed
-
- Ettinger DS, Akerley W, Borghaei H, Chang AC, Cheney RT, Chirieac LR, et al. Non-small cell lung cancer. J Natl Compr Canc Netw. 2012;10:1236–71. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30. - PubMed
-
- Goldstraw P, Chansky K, Crowley J, Rami-Porta R, Asamura H, Eberhardt WEE, et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol. 2016;11:39–51. - PubMed
-
- Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228–47. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
