

A signature of circulating inflammatory proteins and development of end-stage renal disease in diabetes
- PMID: 31011203
- PMCID: PMC6508971
- DOI: 10.1038/s41591-019-0415-5
A signature of circulating inflammatory proteins and development of end-stage renal disease in diabetes
Abstract
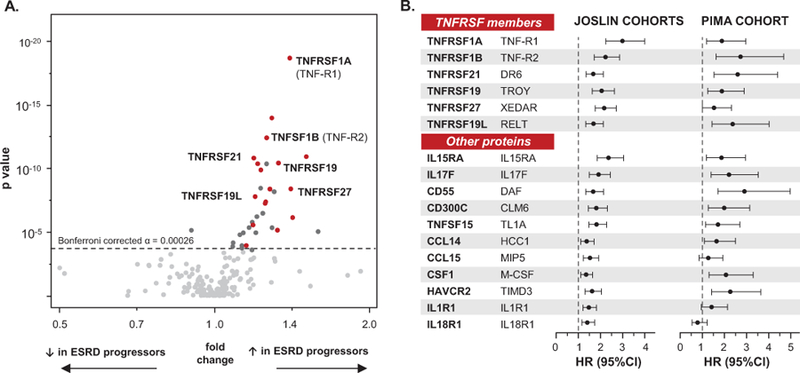
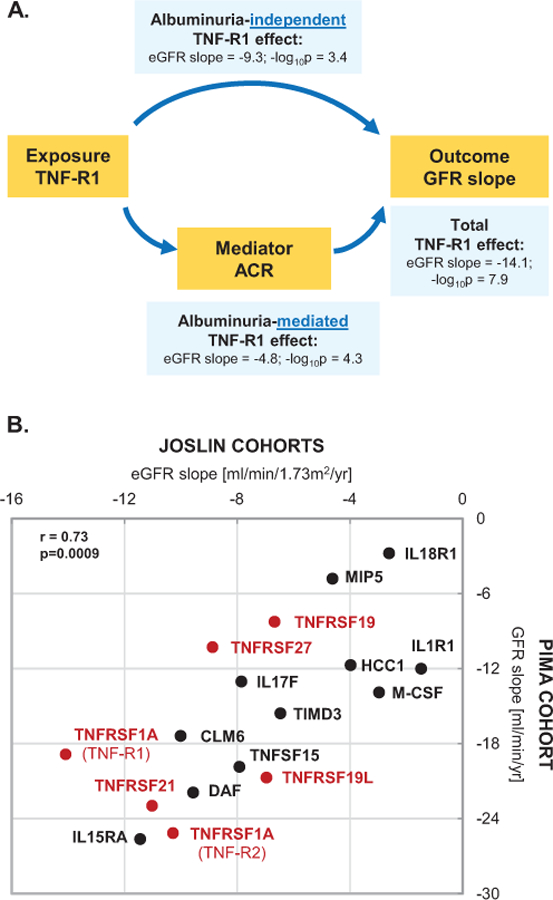
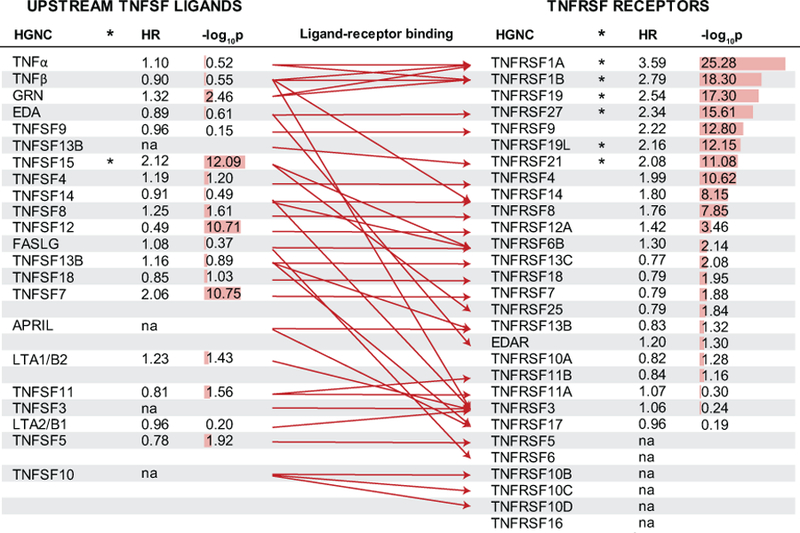
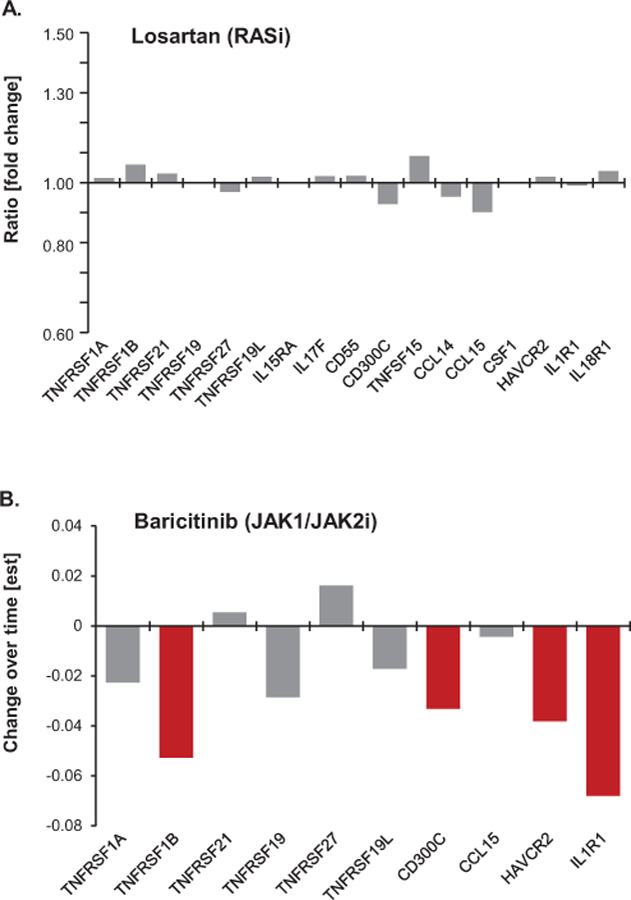
Chronic inflammation is postulated to be involved in the development of end-stage renal disease in diabetes, but which specific circulating inflammatory proteins contribute to this risk remain unknown. To study this, we examined 194 circulating inflammatory proteins in subjects from three independent cohorts with type 1 and type 2 diabetes. In each cohort, we identified an extremely robust kidney risk inflammatory signature (KRIS), consisting of 17 proteins enriched in tumor necrosis factor-receptor superfamily members, that was associated with a 10-year risk of end-stage renal disease. All these proteins had a systemic, non-kidney source. Our prospective study findings provide strong evidence that KRIS proteins contribute to the inflammatory process underlying end-stage renal disease development in both types of diabetes. These proteins point to new therapeutic targets and new prognostic tests to identify subjects at risk of end-stage renal disease, as well as biomarkers to measure responses to treatment of diabetic kidney disease.
Conflict of interest statement
Competing Interest Statement:
ASK and MAN are co-inventors of the TNF-R1 and TNF-R2 patent for predicting risk of ESRD. This patent was licensed by the Joslin Diabetes Center to EKF Diagnostics.
The other authors of this report declare no competing conflicts of interest.
Figures
Comment in
-
A signature of inflammatory proteins associated with ESRD in diabetes.Nat Rev Nephrol. 2019 Jul;15(7):387. doi: 10.1038/s41581-019-0157-0. Nat Rev Nephrol. 2019. PMID: 31053790 No abstract available.
-
Inflammatory proteins in diabetic kidney disease-potential as biomarkers and therapeutic targets.Ann Transl Med. 2019 Sep;7(Suppl 6):S243. doi: 10.21037/atm.2019.08.20. Ann Transl Med. 2019. PMID: 31656822 Free PMC article. No abstract available.
References
-
- Gregg EW, et al. Changes in diabetes-related complications in the United States, 1990–2010. N Engl J Med 370, 1514–1523 (2014). - PubMed
-
- Macisaac RJ, Ekinci EI & Jerums G Markers of and risk factors for the development and progression of diabetic kidney disease. Am J Kidney Dis 63, S39–62 (2014). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
