

Genomic and transcriptomic profiling expands precision cancer medicine: the WINTHER trial
- PMID: 31011205
- PMCID: PMC6599610
- DOI: 10.1038/s41591-019-0424-4
Genomic and transcriptomic profiling expands precision cancer medicine: the WINTHER trial
Abstract
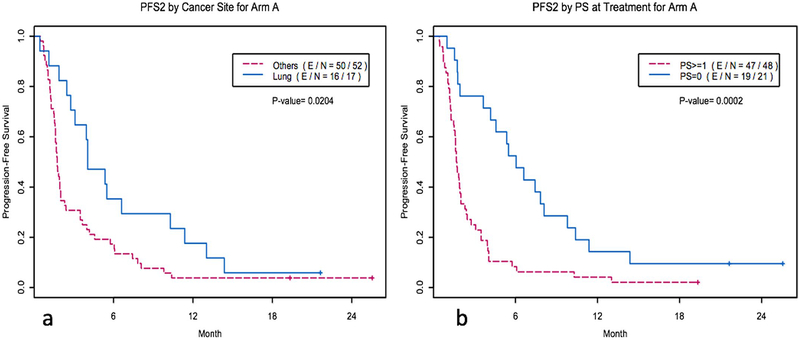
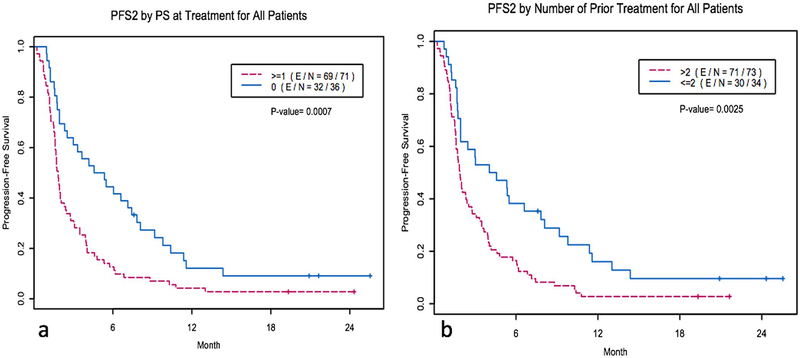
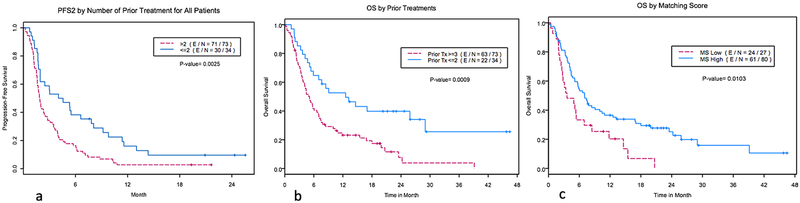
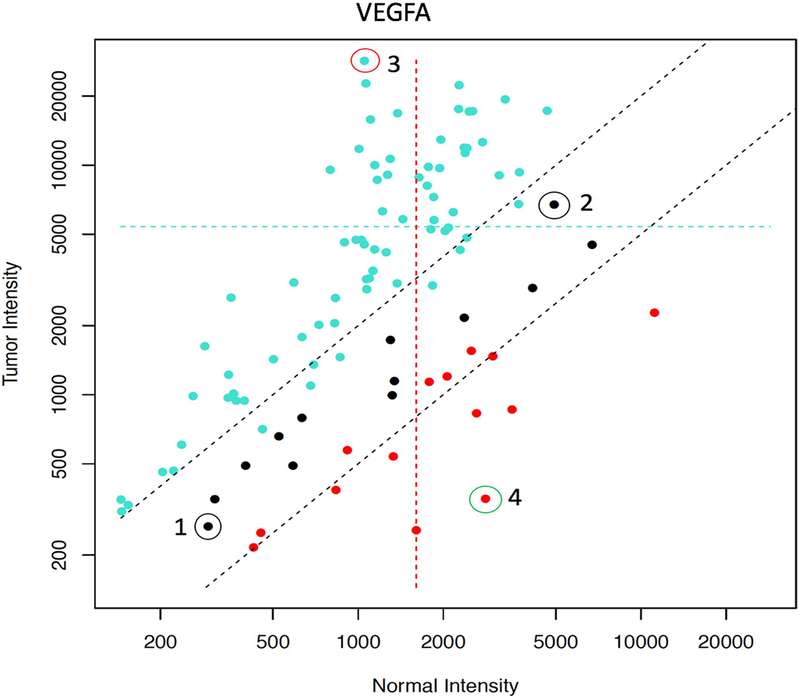
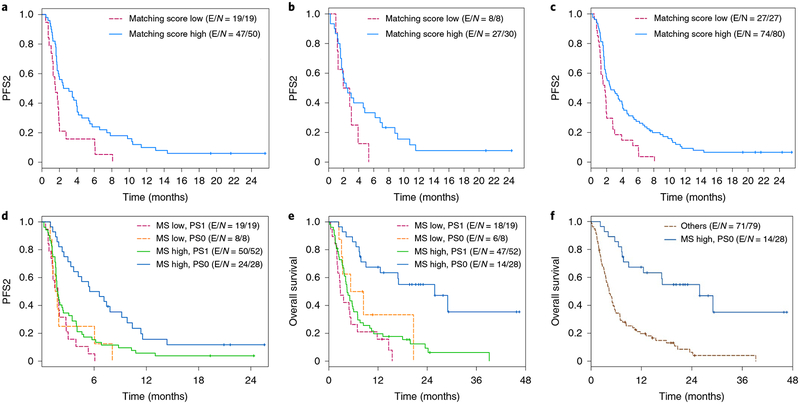
Precision medicine focuses on DNA abnormalities, but not all tumors have tractable genomic alterations. The WINTHER trial ( NCT01856296 ) navigated patients to therapy on the basis of fresh biopsy-derived DNA sequencing (arm A; 236 gene panel) or RNA expression (arm B; comparing tumor to normal). The clinical management committee (investigators from five countries) recommended therapies, prioritizing genomic matches; physicians determined the therapy given. Matching scores were calculated post-hoc for each patient, according to drugs received: for DNA, the number of alterations matched divided by the total alteration number; for RNA, expression-matched drug ranks. Overall, 303 patients consented; 107 (35%; 69 in arm A and 38 in arm B) were evaluable for therapy. The median number of previous therapies was three. The most common diagnoses were colon, head and neck, and lung cancers. Among the 107 patients, the rate of stable disease ≥6 months and partial or complete response was 26.2% (arm A: 23.2%; arm B: 31.6% (P = 0.37)). The patient proportion with WINTHER versus previous therapy progression-free survival ratio of >1.5 was 22.4%, which did not meet the pre-specified primary end point. Fewer previous therapies, better performance status and higher matching score correlated with longer progression-free survival (all P < 0.05, multivariate). Our study shows that genomic and transcriptomic profiling are both useful for improving therapy recommendations and patient outcome, and expands personalized cancer treatment.
Conflict of interest statement
Competing interests
J.Rodon reports non-financial support and reasonable reimbursement for travel from the
Figures


Comment in
-
Molecular profiling in precision medicine oncology.Nat Med. 2019 May;25(5):711-712. doi: 10.1038/s41591-019-0442-2. Nat Med. 2019. PMID: 31036881 No abstract available.
-
Precision Oncology: Three Small Steps Forward.Cancer Cell. 2019 Jun 10;35(6):825-826. doi: 10.1016/j.ccell.2019.05.009. Cancer Cell. 2019. PMID: 31185208 Free PMC article.
-
Studies Show Clinical Utility of Precision Medicine.Cancer Discov. 2019 Aug;9(8):OF8. doi: 10.1158/2159-8290.CD-ND2019-008. Epub 2019 Jun 26. Cancer Discov. 2019. PMID: 31242995
References
-
- Schwaederle M et al. Association of biomarker-based treatment strategies with response rates and progression-free survival in refractory malignant neoplasms: a meta-analysis. JAMA Oncol. 2, 1452–1459 (2016). - PubMed
-
- Tsao MS et al. Erlotinib in lung cancer—molecular and clinical predictors of outcome. N. Engl. J. Med 353, 133–144 (2005). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
