

Gastric Emphysema in a Critically Ill Patient Successfully Treated without Surgery
- PMID: 31011454
- PMCID: PMC6442441
- DOI: 10.1155/2019/1824101
Gastric Emphysema in a Critically Ill Patient Successfully Treated without Surgery
Abstract
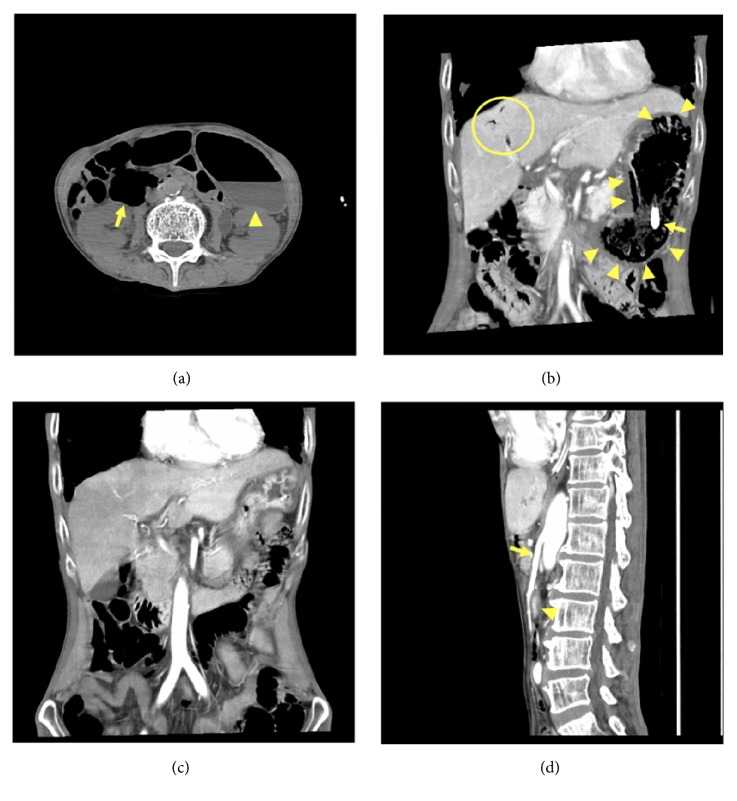
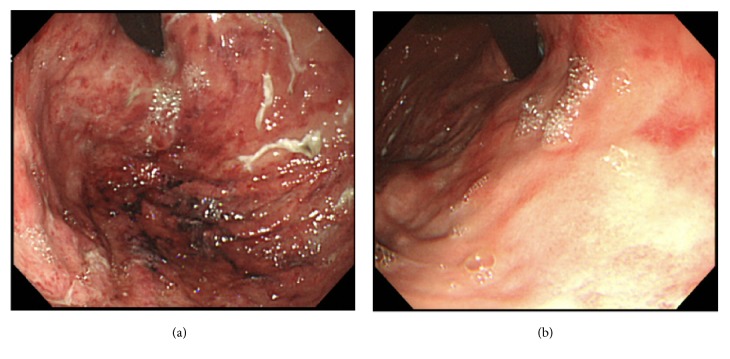
Gastric emphysema is a relatively rare clinical entity caused by injury to the gastric mucosa. A 62-year-old Japanese male with a history of heavy alcohol consumption and smoking was admitted to the emergency intensive care unit due to severe hypercapnic respiratory acidosis. His body mass index was only 12.6. Ten days after initiation of enteral feeding, he complained of abdominal pain. Computed tomography revealed intraluminal air in the distended gastric wall. Esophagogastroduodenoscopy showed diffuse edema, redness, and erosion throughout the stomach. Based on the findings of narrow angle and short distance of the aorta-superior mesenteric artery, the patient was diagnosed with gastric emphysema associated with superior mesenteric artery syndrome. He was successfully managed nonoperatively with treatments including intravenous antibiotics, gastric decompression, and bowel rest. Physicians should be aware of this unusual condition in such critically ill patients complaining of abdominal pain and needing close monitoring and observation to exclude gastric necrosis or perforation.
Figures
Similar articles
-
Gastric intramural and portal venous gas following blunt abdominal injury.Arch Trauma Res. 2013 Aug;2(2):95-6. doi: 10.5812/atr.10866. Epub 2013 Aug 1. Arch Trauma Res. 2013. PMID: 24396802 Free PMC article.
-
Gastric emphysema with portal emphysema due to superior mesenteric artery syndrome developing septic shock: a case report.Acute Med Surg. 2019 Jul 11;6(4):404-407. doi: 10.1002/ams2.440. eCollection 2019 Oct. Acute Med Surg. 2019. PMID: 31592323 Free PMC article.
-
Emphysematous gastritis with delayed gastric perforation.J Gastrointest Surg. 2013 Jul;17(7):1336-8. doi: 10.1007/s11605-013-2141-5. Epub 2013 Jan 10. J Gastrointest Surg. 2013. PMID: 23307314
-
[A case of gastric perforation caused by chestnut bezoars].Nihon Shokakibyo Gakkai Zasshi. 2017;114(10):1830-1835. doi: 10.11405/nisshoshi.114.1830. Nihon Shokakibyo Gakkai Zasshi. 2017. PMID: 28978882 Review. Japanese.
-
Palliative Chemotherapy: Does It Only Provide False Hope? The Role of Palliative Care in a Young Patient With Newly Diagnosed Metastatic Adenocarcinoma.J Adv Pract Oncol. 2017 May-Jun;8(4):382-386. Epub 2017 May 1. J Adv Pract Oncol. 2017. PMID: 30018843 Free PMC article. Review.
Cited by
-
Cytomegalovirus Colitis Followed by Colonic Pseudolipomatosis and Gastric Emphysema in a Post-resuscitation Patient.Intern Med. 2020 Feb 15;59(4):519-525. doi: 10.2169/internalmedicine.3633-19. Epub 2019 Oct 24. Intern Med. 2020. PMID: 31645533 Free PMC article.
-
Emphysematous Gastritis in a Chronic Alcohol User: A Case of Gastric Pneumatosis With Suspected Infectious Etiology.Cureus. 2025 Aug 18;17(8):e90360. doi: 10.7759/cureus.90360. eCollection 2025 Aug. Cureus. 2025. PMID: 40831980 Free PMC article.
-
[Emphysematous gastritis. Report of a case in the elderly].Rev Med Inst Mex Seguro Soc. 2022 Mar 1;60(2):236-241. Rev Med Inst Mex Seguro Soc. 2022. PMID: 35759695 Free PMC article. Spanish.
-
Endoscopic and clinical features of gastric emphysema.Sci Rep. 2024 Jan 25;14(1):2202. doi: 10.1038/s41598-024-52633-z. Sci Rep. 2024. PMID: 38273039 Free PMC article.
References
-
- Lee S., Rutledge JN. Gastric emphysema. The American Journal of Gastroenterology. 1984;79(11):899–904. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
