

The Meta VCI Map consortium for meta-analyses on strategic lesion locations for vascular cognitive impairment using lesion-symptom mapping: Design and multicenter pilot study
- PMID: 31011619
- PMCID: PMC6465616
- DOI: 10.1016/j.dadm.2019.02.007
The Meta VCI Map consortium for meta-analyses on strategic lesion locations for vascular cognitive impairment using lesion-symptom mapping: Design and multicenter pilot study
Abstract
Introduction: The Meta VCI Map consortium performs meta-analyses on strategic lesion locations for vascular cognitive impairment using lesion-symptom mapping. Integration of data from different cohorts will increase sample sizes, to improve brain lesion coverage and support comprehensive lesion-symptom mapping studies.
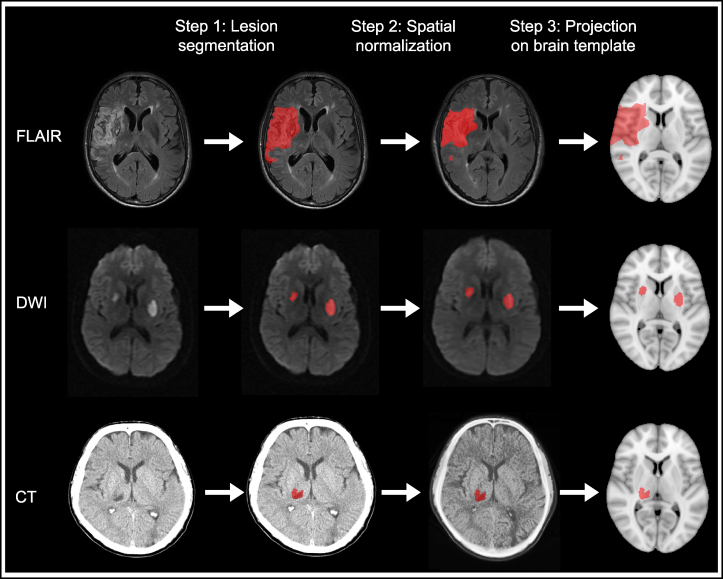
Methods: Cohorts with available imaging on white matter hyperintensities or infarcts and cognitive testing were invited. We performed a pilot study to test the feasibility of multicenter data processing and analysis and determine the benefits to lesion coverage.
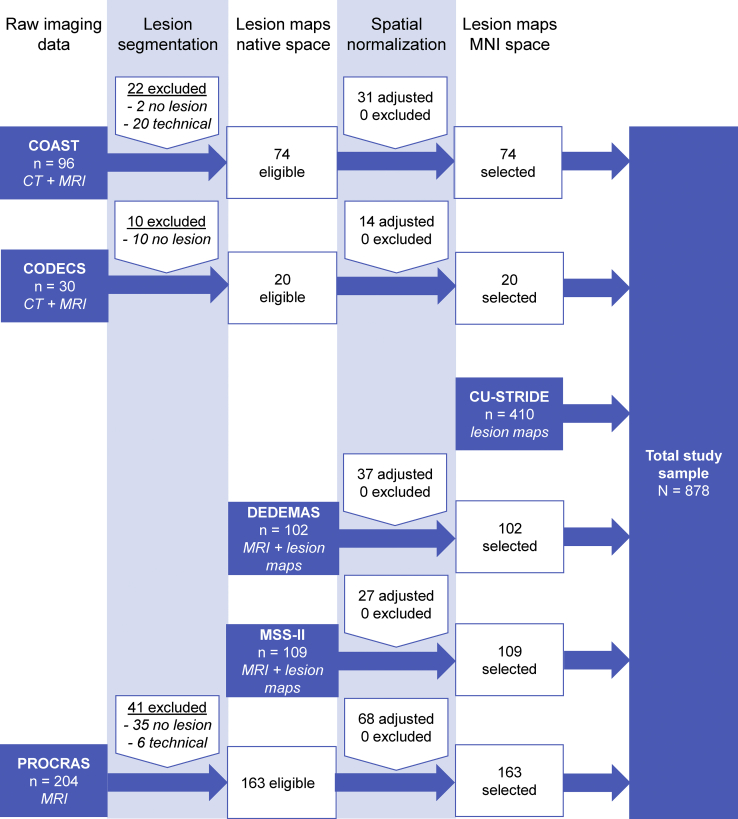
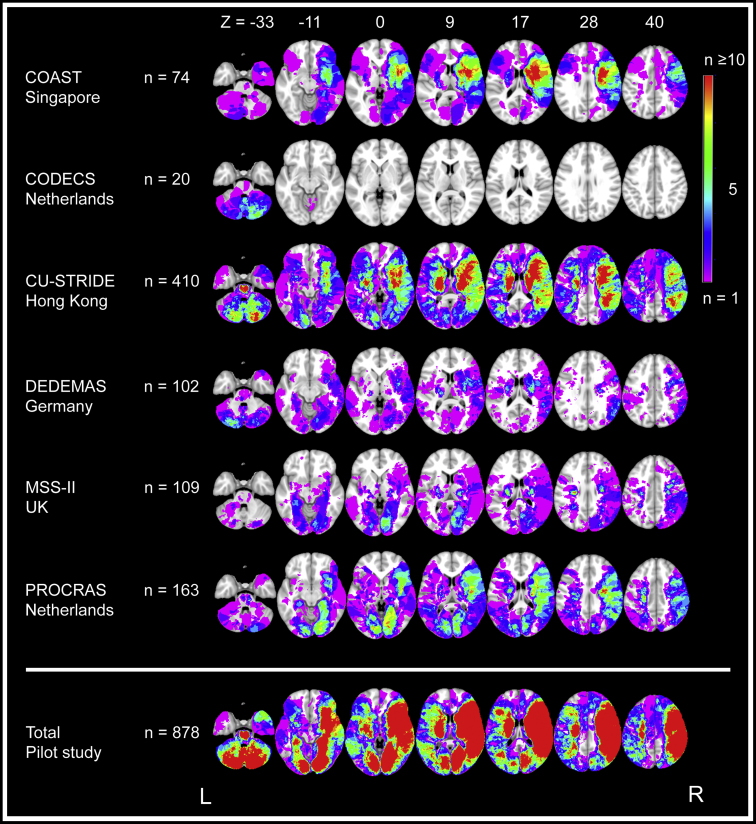
Results: Forty-seven groups have joined Meta VCI Map (stroke n = 7800 patients; memory clinic n = 4900; population-based n = 14,400). The pilot study (six ischemic stroke cohorts, n = 878) demonstrated feasibility of multicenter data integration (computed tomography/magnetic resonance imaging) and achieved marked improvement of lesion coverage.
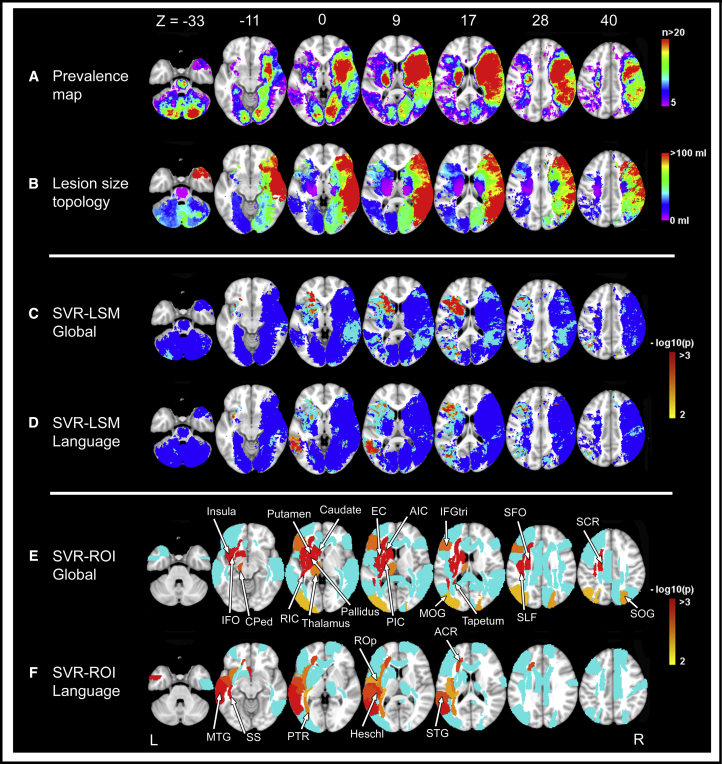
Discussion: Meta VCI Map will provide new insights into the relevance of vascular lesion location for cognitive dysfunction. After the successful pilot study, further projects are being prepared. Other investigators are welcome to join.
Keywords: Cerebrovascular disease; Consortium; Data harmonization; Lesion location; Lesion-symptom mapping; Small vessel disease; Stroke; Support vector regression; Vascular cognitive impairment.
Figures
References
-
- Prins N.D., Scheltens P. White matter hyperintensities, cognitive impairment and dementia: An update. Nat Rev Neurol. 2015;11:157–165. - PubMed
-
- Biesbroek J.M., Weaver N.A., Biessels G.J. Lesion location and cognitive impact of cerebral small vessel disease. Clin Sci. 2017;131:715–728. - PubMed
-
- Rorden C., Karnath H.O. Using human brain lesions to infer function: A relic from a past era in the fMRI age? Nat Rev Neurosci. 2004;5:812–819. - PubMed
-
- Duering M., Zieren N., Hervé D., Jouvent E., Reyes S., Peters N. Strategic role of frontal white matter tracts in vascular cognitive impairment: A voxel-based lesion-symptom mapping study in CADASIL. Brain. 2011;134:2366–2375. - PubMed
Grants and funding
- UH3 NS100605/NS/NINDS NIH HHS/United States
- R01 AG054076/AG/NIA NIH HHS/United States
- RF1 AG059421/AG/NIA NIH HHS/United States
- MC_UU_00019/1/MRC_/Medical Research Council/United Kingdom
- G0300623/MRC_/Medical Research Council/United Kingdom
- MC_UU_00019/3/MRC_/Medical Research Council/United Kingdom
- U01 AG049505/AG/NIA NIH HHS/United States
- MR/J006971/1/MRC_/Medical Research Council/United Kingdom
- R01 NS017950/NS/NINDS NIH HHS/United States
- P30 AG066546/AG/NIA NIH HHS/United States
- U01 AG052409/AG/NIA NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
- P30 AG010129/AG/NIA NIH HHS/United States