

Safety profile of the RTS,S/AS01 malaria vaccine in infants and children: additional data from a phase III randomized controlled trial in sub-Saharan Africa
- PMID: 31012786
- PMCID: PMC6816384
- DOI: 10.1080/21645515.2019.1586040
Safety profile of the RTS,S/AS01 malaria vaccine in infants and children: additional data from a phase III randomized controlled trial in sub-Saharan Africa
Abstract
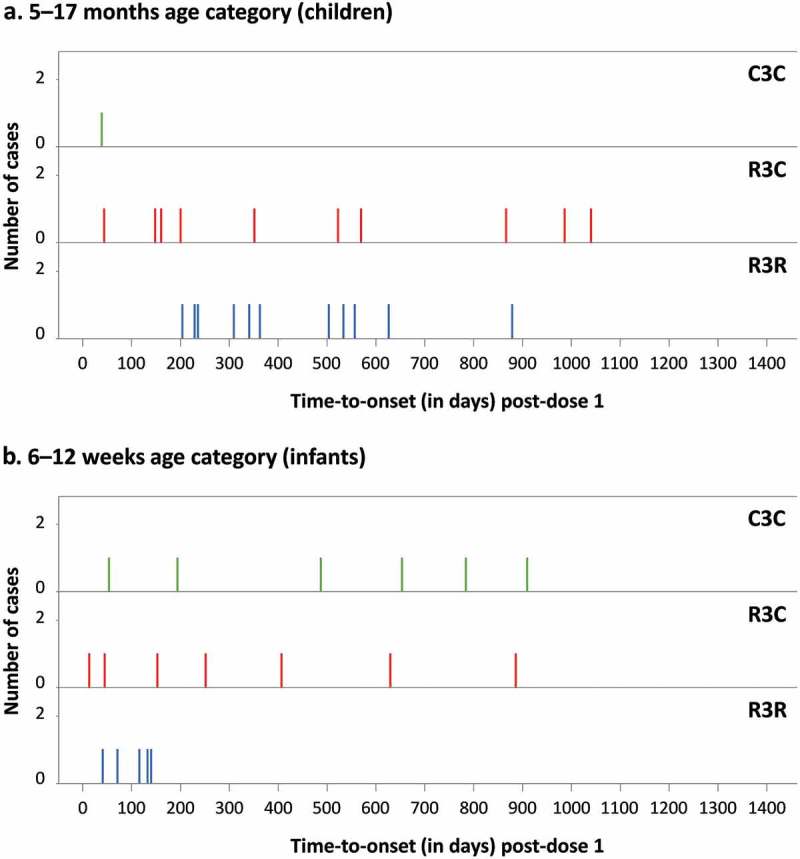
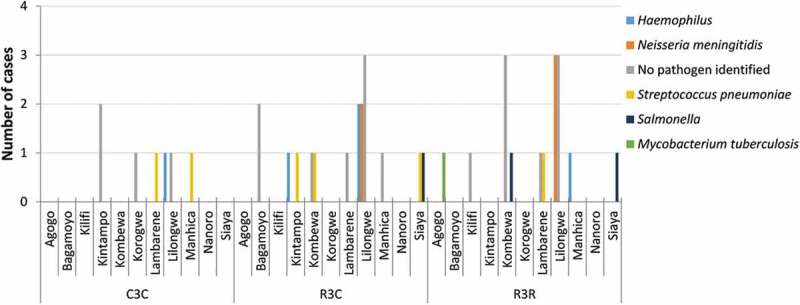
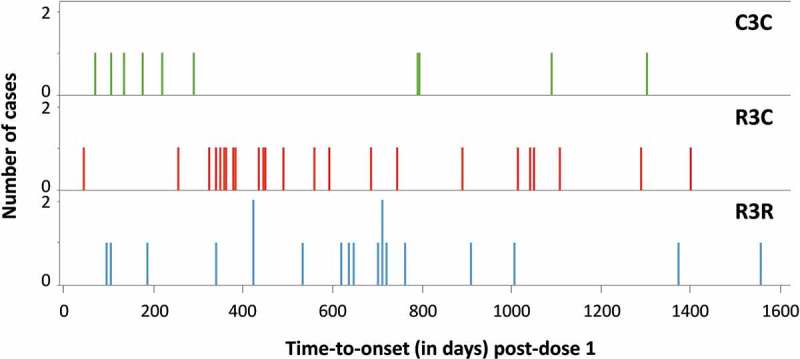
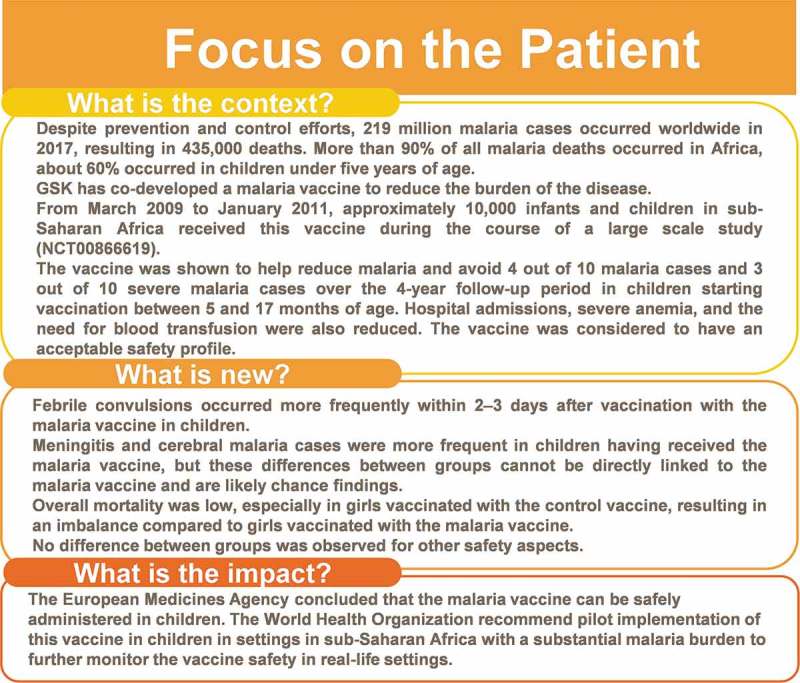
A phase III, double-blind, randomized, controlled trial (NCT00866619) in sub-Saharan Africa showed RTS,S/AS01 vaccine efficacy against malaria. We now present in-depth safety results from this study. 8922 children (enrolled at 5-17 months) and 6537 infants (enrolled at 6-12 weeks) were 1:1:1-randomized to receive 4 doses of RTS,S/AS01 (R3R) or non-malaria control vaccine (C3C), or 3 RTS,S/AS01 doses plus control (R3C). Aggregate safety data were reviewed by a multi-functional team. Severe malaria with Blantyre Coma Score ≤2 (cerebral malaria [CM]) and gender-specific mortality were assessed post-hoc. Serious adverse event (SAE) and fatal SAE incidences throughout the study were 24.2%-28.4% and 1.5%-2.5%, respectively across groups; 0.0%-0.3% of participants reported vaccination-related SAEs. The incidence of febrile convulsions in children was higher during the first 2-3 days post-vaccination with RTS,S/AS01 than with control vaccine, consistent with the time window of post-vaccination febrile reactions in this study (mostly the day after vaccination). A statistically significant numerical imbalance was observed for meningitis cases in children (R3R: 11, R3C: 10, C3C: 1) but not in infants. CM cases were more frequent in RTS,S/AS01-vaccinated children (R3R: 19, R3C: 24, C3C: 10) but not in infants. All-cause mortality was higher in RTS,S/AS01-vaccinated versus control girls (2.4% vs 1.3%, all ages) in our setting with low overall mortality. The observed meningitis and CM signals are considered likely chance findings, that - given their severity - warrant further evaluation in phase IV studies and WHO-led pilot implementation programs to establish the RTS,S/AS01 benefit-risk profile in real-life settings.
Keywords: (5–10): Malaria; RTS,S/AS01 vaccine; cerebral malaria; febrile convulsions; meningitis; safety.
Figures
References
-
- World Health Organization World Malaria Report 2018. Geneva, Switzerland: World Health Organization; 2018. [accessed 14December, 2018] https://www.who.int/malaria/publications/world-malaria-report-2018/repor....
-
- Asante KP, Abdulla S, Agnandji S, Lyimo J, Vekemans J, Soulanoudjingar S, Owusu R, Shomari M, Leach A, Jongert E, et al. Safety and efficacy of the RTS,S/AS01E candidate malaria vaccine given with expanded-programme-on-immunisation vaccines: 19 month follow-up of a randomised, open-label, phase 2 trial. Lancet Infect Dis. 2011;11(10):741–49. doi: 10.1016/S1473-3099(11)70100-1. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources