

Association of State Medicaid Expansion Status With Low Birth Weight and Preterm Birth
- PMID: 31012935
- PMCID: PMC6487545
- DOI: 10.1001/jama.2019.3678
Association of State Medicaid Expansion Status With Low Birth Weight and Preterm Birth
Abstract
Importance: Low birth weight and preterm birth are associated with adverse consequences including increased risk of infant mortality and chronic health conditions. Black infants are more likely than white infants to be born prematurely, which has been associated with disparities in infant mortality and other chronic conditions.
Objective: To evaluate whether Medicaid expansion was associated with changes in rates of low birth weight and preterm birth outcomes, both overall and by race/ethnicity.
Design, setting, and participants: Using US population-based data from the National Center for Health Statistics Birth Data Files (2011-2016), difference-in-differences (DID) and difference-in-difference-in-differences (DDD) models were estimated using multivariable linear probability regressions to compare birth outcomes among infants in Medicaid expansion states relative to non-Medicaid expansion states and changes in relative disparities among racial/ethnic minorities for singleton live births to women aged 19 years and older.
Exposures: State Medicaid expansion status and racial/ethnic category.
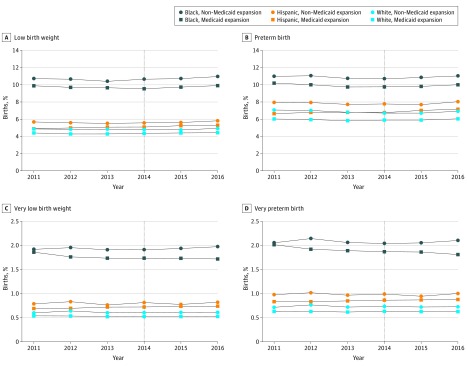
Main outcomes and measures: Preterm birth (<37 weeks' gestation), very preterm birth (<32 weeks' gestation), low birth weight (<2500 g), and very low birth weight (<1500 g).
Results: The final sample of 15 631 174 births (white infants: 8 244 924, black infants: 2 201 658, and Hispanic infants: 3 944 665) came from the District of Columbia and 18 states that expanded Medicaid (n = 8 530 751) and 17 states that did not (n = 7 100 423). In the DID analyses, there were no significant changes in preterm birth in expansion relative to nonexpansion states (preexpansion to postexpansion period, 6.80% to 6.67% [difference: -0.12] vs 7.86% to 7.78% [difference: -0.08]; adjusted DID: 0.00 percentage points [95% CI, -0.14 to 0.15], P = .98), very preterm birth (0.87% to 0.83% [difference: -0.04] vs 1.02% to 1.03% [difference: 0.01]; adjusted DID: -0.02 percentage points [95% CI, -0.05 to 0.02], P = .37), low birth weight (5.41% to 5.36% [difference: -0.05] vs 6.06% to 6.18% [difference: 0.11]; adjusted DID: -0.08 percentage points [95% CI, -0.20 to 0.04], P = .20), or very low birth weight (0.76% to 0.72% [difference: -0.03] vs 0.88% to 0.90% [difference: 0.02]; adjusted DID: -0.03 percentage points [95% CI, -0.06 to 0.01], P = .14). Disparities for black infants relative to white infants in Medicaid expansion states compared with nonexpansion states declined for all 4 outcomes, indicated by a negative DDD coefficient for preterm birth (-0.43 percentage points [95% CI, -0.84 to -0.02], P = .05), very preterm birth (-0.14 percentage points [95% CI, -0.26 to -0.02], P = .03), low birth weight (-0.53 percentage points [95% CI, -0.96 to -0.10], P = .02), and very low birth weight (-0.13 percentage points [95% CI, -0.25 to -0.01], P = .04). There were no changes in relative disparities for Hispanic infants.
Conclusions and relevance: Based on data from 2011-2016, state Medicaid expansion was not significantly associated with differences in rates of low birth weight or preterm birth outcomes overall, although there were significant improvements in relative disparities for black infants compared with white infants in states that expanded Medicaid vs those that did not.
Conflict of interest statement
Figures
Comment in
-
Medicaid Expansion and Birth Outcomes.JAMA. 2019 Apr 23;321(16):1609. doi: 10.1001/jama.2019.3824. JAMA. 2019. PMID: 31012913 No abstract available.
-
Perinatal Outcomes in Medicaid Expansion and Nonexpansion States Among Hispanic Women.JAMA. 2019 Sep 3;322(9):893-894. doi: 10.1001/jama.2019.9825. JAMA. 2019. PMID: 31479131 No abstract available.
References
-
- Matthews TJ, MacDorman MF, Thoma ME. Infant mortality statistics from the 2013 period linked birth/infant death data set. Natl Vital Stat Rep. 2015;64(9):1-30. - PubMed
-
- Behrman RE, Butler AS; Institute of Medicine, Committee on Understanding Premature Birth and Assuring Healthy Outcomes . Preterm Birth: Causes, Consequences, and Prevention. Washington, DC: National Academies Press; 2007. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
