

Lay health supporters aided by mobile text messaging to improve adherence, symptoms, and functioning among people with schizophrenia in a resource-poor community in rural China (LEAN): A randomized controlled trial
- PMID: 31013275
- PMCID: PMC6478272
- DOI: 10.1371/journal.pmed.1002785
Lay health supporters aided by mobile text messaging to improve adherence, symptoms, and functioning among people with schizophrenia in a resource-poor community in rural China (LEAN): A randomized controlled trial
Abstract
Background: Schizophrenia is a leading cause of disability, and a shift from facility- to community-based care has been proposed to meet the resource challenges of mental healthcare in low- and middle-income countries. We hypothesized that the addition of mobile texting would improve schizophrenia care in a resource-poor community setting compared with a community-based free-medicine program alone.
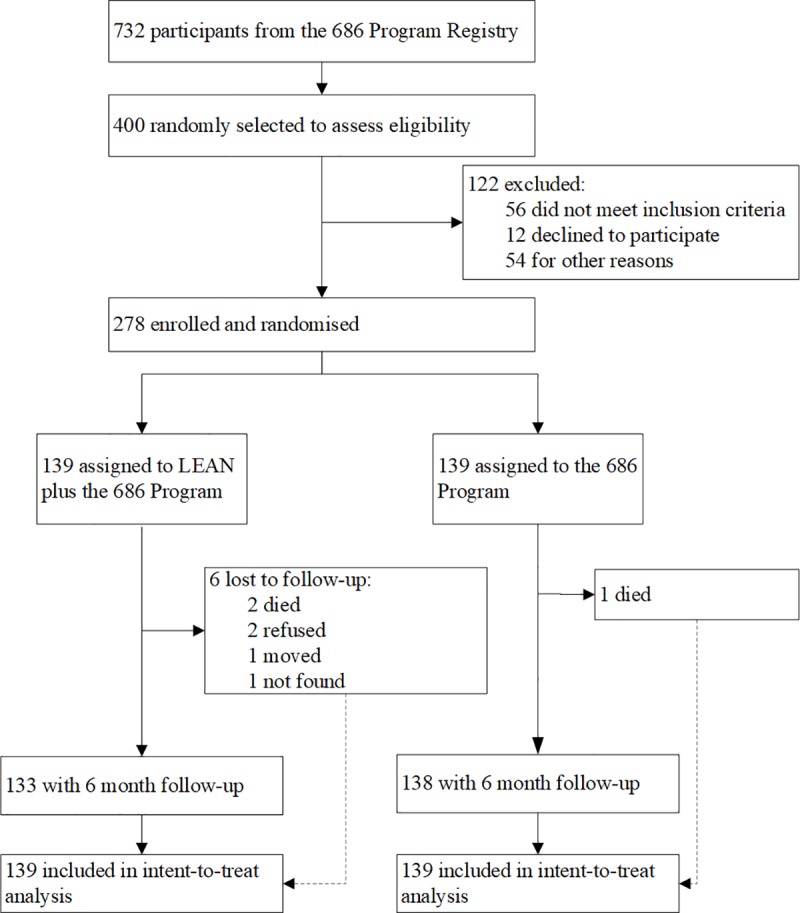
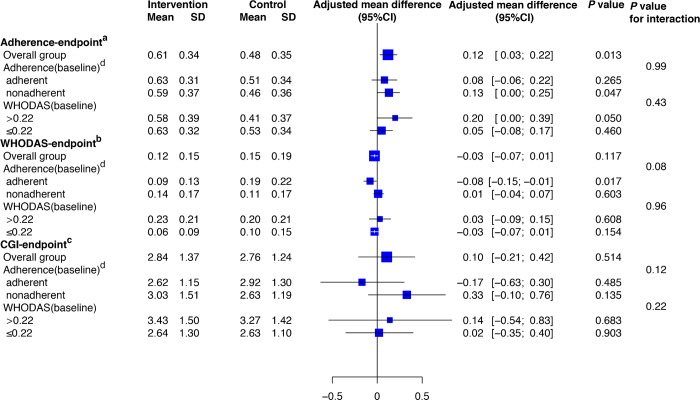
Methods and findings: In this 2-arm randomized controlled trial, 278 community-dwelling villagers (patient participants) were randomly selected from people with schizophrenia from 9 townships of Hunan, China, and were randomized 1:1 into 2 groups. The program participants were recruited between May 1, 2015, and August 31, 2015, and the intervention and follow-up took place between December 15, 2015, and July 1, 2016. Baseline characteristics of the 2 groups were similar. The patients were on average 46 years of age, had 7 years of education, had a duration of schizophrenia of 18 years with minimal to mild symptoms and nearly one-fifth loss of functioning, and were mostly living with family (95%) and had low incomes. Both the intervention and the control groups received a nationwide community-based mental health program that provided free antipsychotic medications. The patient participants in the intervention group also received LEAN (Lay health supporters, E-platform, Award, and iNtegration), a program that featured recruitment of a lay health supporter and text messages for medication reminders, health education, monitoring of early signs of relapses, and facilitated linkage to primary healthcare. The primary outcome was medication adherence (proportion of dosages taken) assessed by 2 unannounced home-based pill counts 30 days apart at the 6-month endpoint. The secondary and other outcomes included patient symptoms, functioning, relapses, re-hospitalizations, death for any reason, wandering away without notifying anyone, violence against others, damaging goods, and suicide. Intent-to-treat analysis was used. Missing data were handled with multiple imputations. In total, 271 out of 278 patient participants were successfully followed up for outcome assessment. Medication adherence was 0.48 in the control group and 0.61 in the intervention group (adjusted mean difference [AMD] 0.12 [95% CI 0.03 to 0.22]; p = 0.013; effect size 0.38). Among secondary and other outcomes we noted substantial reduction in the risk of relapse (26 [21.7%] of 120 interventional participants versus 40 [34.2%] of 117 controls; relative risk 0.63 [95% CI 0.42 to 0.97]; number needed to treat [NNT] 8.0) and re-hospitalization (9 [7.3%] of 123 interventional participants versus 25 [20.5%] of 122 controls; relative risk 0.36 [95% CI 0.17 to 0.73]; NNT 7.6). The program showed no statistical difference in all other outcomes. During the course of the program, 2 participants in the intervention group and 1 in the control group died. The limitations of the study include its lack of a full economic analysis, lack of individual tailoring of the text messages, the relatively short 6-month follow-up, and the generalizability constraint of the Chinese context.
Conclusions: The addition of texting to patients and their lay health supporters in a resource-poor community setting was more effective than a free-medicine program alone in improving medication adherence and reducing relapses and re-hospitalizations. Future studies may test the effectiveness of customization of the texting to individual patients.
Trial registration: Chinese Clinical Trial Registry ChiCTR-ICR-15006053.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Institute for Health Metrics and Evaluation. GBD compare Seattle: Institute for Health Metrics and Evaluation; 2019. [cited 2019 Mar 26]. Available from: http://www.healthdata.org/data-visualization/gbd-compare.
-
- Rice DP, Miller LS. The economic burden of schizophrenia: conceptual and methodological issues, and cost estimates In: Moscarelli M, Rupp A, Sartorius N, editors. Handbook of mental health economics and health policy. Vol. 1. Schizophrenia . Oxford: John Wiley & Sons; 1996. pp. 321–34.
-
- Chan M. Mental health and development: targeting people with mental health conditions as a vulnerable group Geneva: World Health Organization; 2010. [cited 2019 Jan 28]. Available from: https://www.who.int/mental_health/policy/mhtargeting/en/.
-
- World Health Organization. mhGAP: Mental Health Gap Action Programme—scaling up care for mental, neurological and substance use disorders Geneva: World Health Organization; 2008. [cited 2019 Jan 28]. Available from: https://www.who.int/mental_health/mhgap_final_english.pdf?ua=1. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
