

Socioeconomic position and use of healthcare in the last year of life: A systematic review and meta-analysis
- PMID: 31013279
- PMCID: PMC6478269
- DOI: 10.1371/journal.pmed.1002782
Socioeconomic position and use of healthcare in the last year of life: A systematic review and meta-analysis
Erratum in
-
Correction: Socioeconomic position and use of healthcare in the last year of life: A systematic review and meta-analysis.PLoS Med. 2019 Jul 18;16(7):e1002878. doi: 10.1371/journal.pmed.1002878. eCollection 2019 Jul. PLoS Med. 2019. PMID: 31318866 Free PMC article.
Abstract
Background: Low socioeconomic position (SEP) is recognized as a risk factor for worse health outcomes. How socioeconomic factors influence end-of-life care, and the magnitude of their effect, is not understood. This review aimed to synthesise and quantify the associations between measures of SEP and use of healthcare in the last year of life.
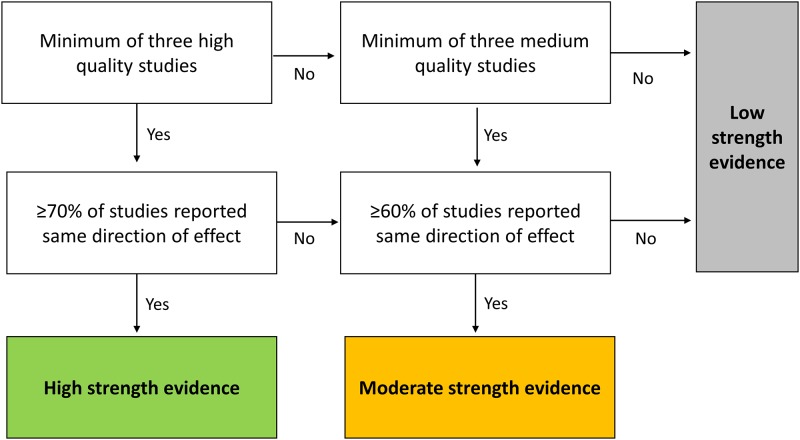
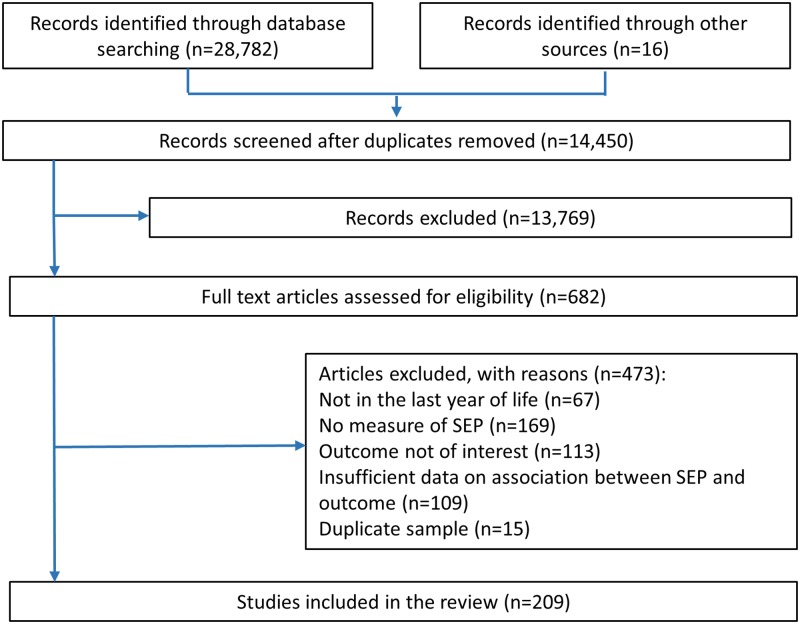
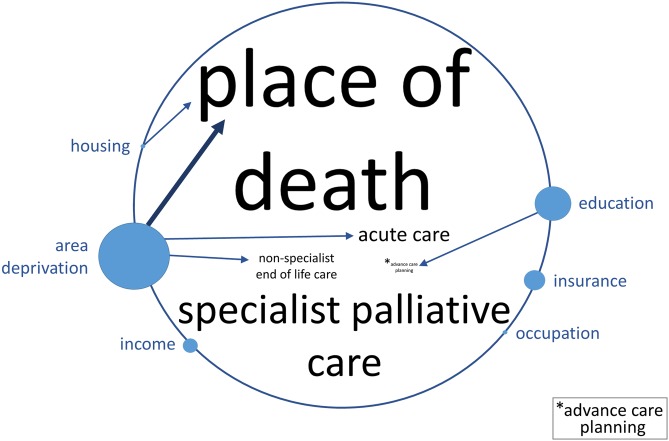
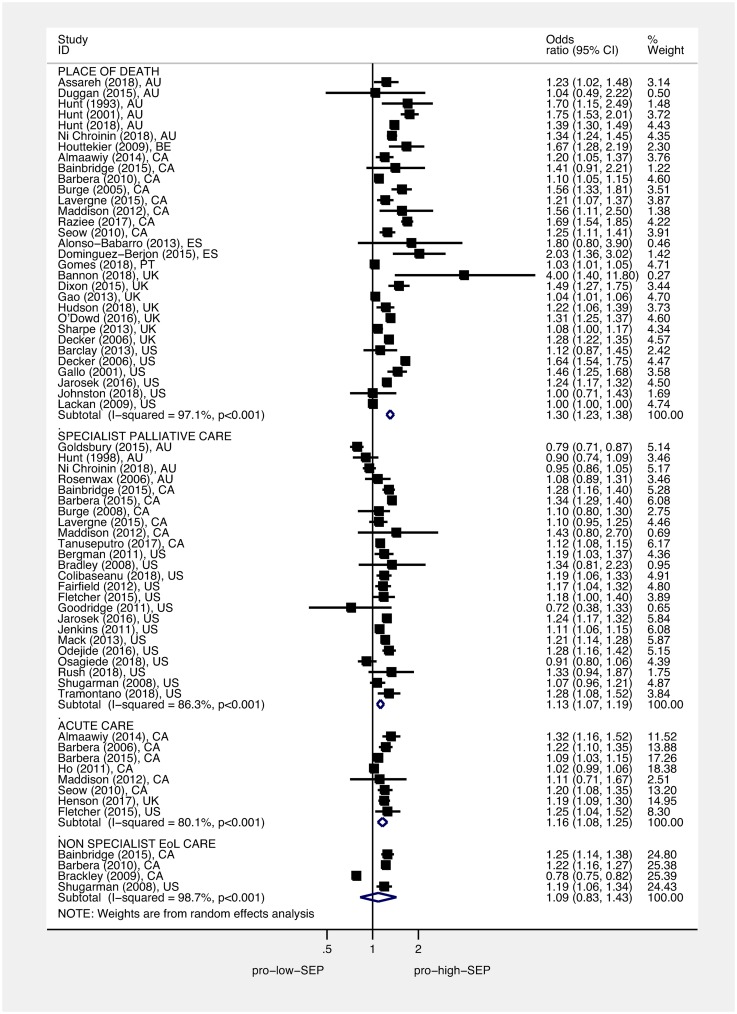
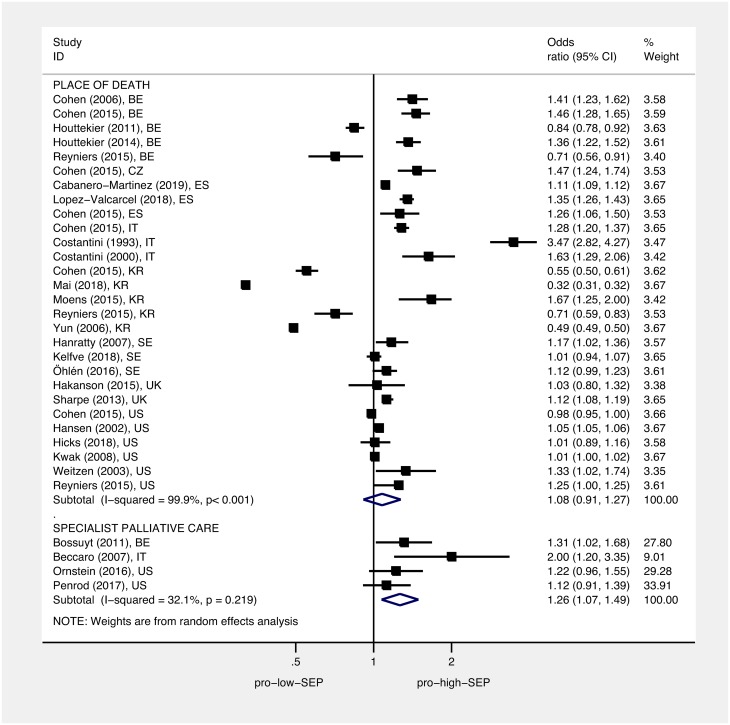
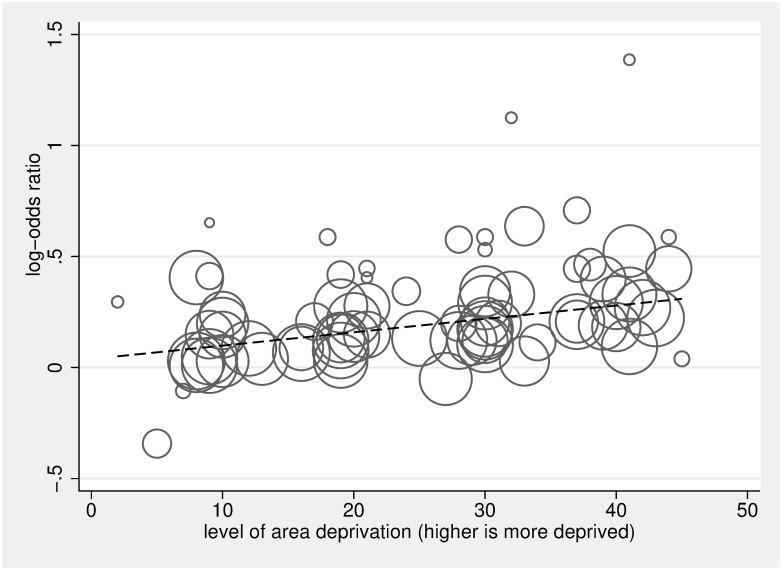
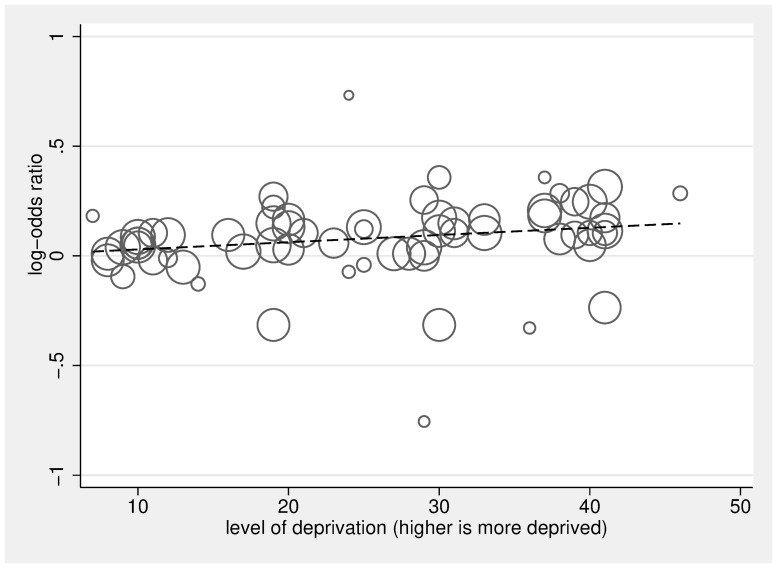
Methods and findings: MEDLINE, EMBASE, PsycINFO, CINAHL, and ASSIA databases were searched without language restrictions from inception to 1 February 2019. We included empirical observational studies from high-income countries reporting an association between SEP (e.g., income, education, occupation, private medical insurance status, housing tenure, housing quality, or area-based deprivation) and place of death, plus use of acute care, specialist and nonspecialist end-of-life care, advance care planning, and quality of care in the last year of life. Methodological quality was evaluated using the Newcastle-Ottawa Quality Assessment Scale (NOS). The overall strength and direction of associations was summarised, and where sufficient comparable data were available, adjusted odds ratios (ORs) were pooled and dose-response meta-regression performed. A total of 209 studies were included (mean NOS quality score of 4.8); 112 high- to medium-quality observational studies were used in the meta-synthesis and meta-analysis (53.5% from North America, 31.0% from Europe, 8.5% from Australia, and 7.0% from Asia). Compared to people living in the least deprived neighbourhoods, people living in the most deprived neighbourhoods were more likely to die in hospital versus home (OR 1.30, 95% CI 1.23-1.38, p < 0.001), to receive acute hospital-based care in the last 3 months of life (OR 1.16, 95% CI 1.08-1.25, p < 0.001), and to not receive specialist palliative care (OR 1.13, 95% CI 1.07-1.19, p < 0.001). For every quintile increase in area deprivation, hospital versus home death was more likely (OR 1.07, 95% CI 1.05-1.08, p < 0.001), and not receiving specialist palliative care was more likely (OR 1.03, 95% CI 1.02-1.05, p < 0.001). Compared to the most educated (qualifications or years of education completed), the least educated people were more likely to not receive specialist palliative care (OR 1.26, 95% CI 1.07-1.49, p = 0.005). The observational nature of the studies included and the focus on high-income countries limit the conclusions of this review.
Conclusions: In high-income countries, low SEP is a risk factor for hospital death as well as other indicators of potentially poor-quality end-of-life care, with evidence of a dose response indicating that inequality persists across the social stratum. These findings should stimulate widespread efforts to reduce socioeconomic inequality towards the end of life.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Marmot M. The health gap: The challenge of an unequal world. The Lancet. 2015;386(10011):2442–4. - PubMed
-
- Marmot M. 2010. Fair Society, Healthy Lives: The Marmot Review: strategic review of health inequalities in England post-2010.
-
- WHO. A conceptual framework for action on the social determinants of health: social determinants of health discussion paper 2. World Health Organisation, Commission on the Social Determinants of Health. 2010.
-
- De Schreye R, Houttekier D, Deliens L, Cohen J. Developing indicators of appropriate and inappropriate end-of-life care in people with Alzheimer’s disease, cancer or chronic obstructive pulmonary disease for population-level administrative databases: A RAND/UCLA appropriateness study. Palliative Medicine. 2017;31(10):932–45. 10.1177/0269216317705099 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
