

Coronary Microcirculation Downstream Non-Infarct-Related Arteries in the Subacute Phase of Myocardial Infarction: Implications for Physiology-Guided Revascularization
- PMID: 31014181
- PMCID: PMC6512122
- DOI: 10.1161/JAHA.118.011534
Coronary Microcirculation Downstream Non-Infarct-Related Arteries in the Subacute Phase of Myocardial Infarction: Implications for Physiology-Guided Revascularization
Abstract
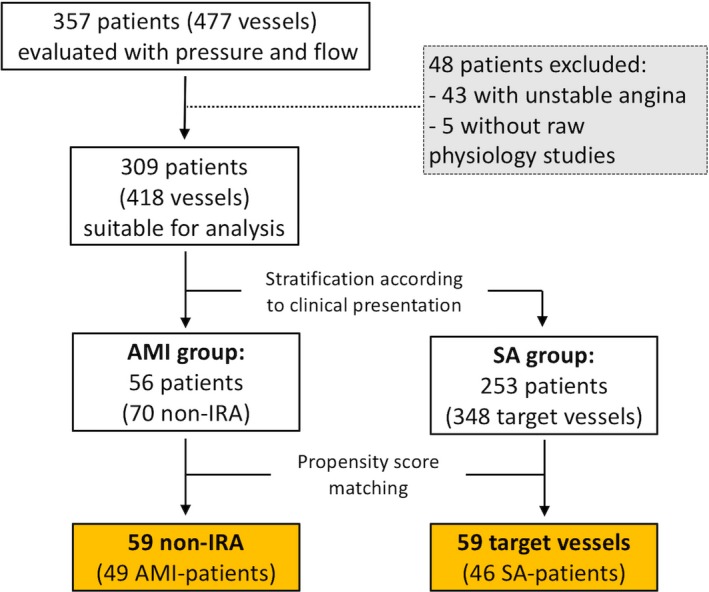
Background Concerns exist about reliability of pressure-wire-guided coronary revascularization of non-infarct-related arteries (non- IRA ). We investigated whether physiological assessment of non- IRA during the subacute phase of myocardial infarction might be flawed by microcirculatory dysfunction. Methods and Results We analyzed non- IRA that underwent fractional flow reserve, coronary flow reserve, and the index of microcirculatory resistance assessment. Microcirculation and hyperemic response were evaluated in 49 acute myocardial infarction patients (59 non- IRA ) and compared with a matched control group of 46 stable angina ( SA ) patients (59 vessels). Time between acute myocardial infarction to physiological interrogation was 5.9±2.4 days. Fractional flow reserve was similar in both groups (0.79±0.11 in non- IRA versus 0.80±0.13 in SA vessels, P=0.527). Lower coronary flow reserve values were found in non- IRA compared with SA vessels (1.77 [1.25-2.76] versus 2.44 [1.63-4.00], P=0.018), primarily driven by an increased baseline flow in non- IRA (rest mean transit time 0.58 [0.32-0.83] versus 0.65 s [0.39-1.20], P=0.045), whereas the hyperemic flow was similar (hyperemic mean transit time 0.26 [0.20-0.42] versus 0.26 s [0.18-0.35], P=0.873). No differences were found regarding index of microcirculatory resistance (15.6 [10.4-21.8] in non- IRA versus 16.7 [11.6-23.6] U in SA vessels, P=0.559). During adenosine infusion, the hyperemic response was similar in both groups (non- IRA versus SA vessels) in terms of the resistive reserve ratio (3.1±2.1 versus 3.7±2.2, P=0.118). Conclusions In the subacute phase of myocardial infarction, non- IRA show an increased baseline flow that may cause abnormal coronary flow reserve despite preserved hyperemic flow. In non- IRA , microcirculatory resistance and adenosine-induced hyperemic response are similar to those found in SA patients. From a physiological perspective, these findings support the use of fractional flow reserve to interrogate non- IRA during the subacute phase of myocardial infarction.
Keywords: coronary flow reserve; coronary microcirculation; fractional flow reserve; microcirculatory resistance; non‐infarct‐related arteries.
Figures






Comment in
-
Robustness of Fractional Flow Reserve for Lesion Assessment in Non-Infarct-Related Arteries of Patients With Myocardial Infarction.J Am Heart Assoc. 2019 May 7;8(9):e012456. doi: 10.1161/JAHA.119.012456. J Am Heart Assoc. 2019. PMID: 31014179 Free PMC article.
Similar articles
-
Coronary Circulatory Indexes in Non-Infarct-Related Vascular Territories in a Porcine Acute Myocardial Infarction Model.JACC Cardiovasc Interv. 2020 May 25;13(10):1155-1167. doi: 10.1016/j.jcin.2020.03.006. JACC Cardiovasc Interv. 2020. PMID: 32438986
-
Vasodilatory capacity of the coronary microcirculation is preserved in selected patients with non-ST-segment-elevation myocardial infarction.Circ Cardiovasc Interv. 2013 Jun;6(3):231-6. doi: 10.1161/CIRCINTERVENTIONS.112.000180. Epub 2013 Jun 11. Circ Cardiovasc Interv. 2013. PMID: 23756697
-
Interpretation of fractional flow reserve in ST-elevation myocardial infarction culprit lesions.Coron Artery Dis. 2015 Sep;26(6):495-502. doi: 10.1097/MCA.0000000000000278. Coron Artery Dis. 2015. PMID: 26086865
-
Meta-analysis of fractional flow reserve guided complete revascularization versus infarct related artery only revascularization in patients with ST-elevation myocardial infarction and multivessel coronary artery disease.Coron Artery Dis. 2019 Sep;30(6):393-397. doi: 10.1097/MCA.0000000000000740. Coron Artery Dis. 2019. PMID: 31094897
-
Instantaneous wave-free ratio as an alternative to fractional flow reserve in assessment of moderate coronary stenoses: A meta-analysis of diagnostic accuracy studies.Cardiovasc Revasc Med. 2018 Jul-Aug;19(5 Pt B):613-620. doi: 10.1016/j.carrev.2017.12.014. Epub 2017 Dec 27. Cardiovasc Revasc Med. 2018. PMID: 29371084 Review.
Cited by
-
Angiography-derived index of microcirculatory resistance as a novel, pressure-wire-free tool to assess coronary microcirculation in ST elevation myocardial infarction.Int J Cardiovasc Imaging. 2020 Aug;36(8):1395-1406. doi: 10.1007/s10554-020-01831-7. Epub 2020 May 14. Int J Cardiovasc Imaging. 2020. PMID: 32409977 Free PMC article.
-
Practical Application of Coronary Physiologic Assessment: Asia-Pacific Expert Consensus Document: Part 2.JACC Asia. 2023 Sep 12;3(6):825-842. doi: 10.1016/j.jacasi.2023.07.004. eCollection 2023 Dec. JACC Asia. 2023. PMID: 38155788 Free PMC article. Review.
-
[Functional assessment of coronary stenosis: alternative hyperemic, nonhyperemic, and angiographic indexes].REC Interv Cardiol. 2024 Jun 13;6(3):224-234. doi: 10.24875/RECIC.M24000446. eCollection 2024 Jul-Sep. REC Interv Cardiol. 2024. PMID: 40415782 Free PMC article. Review. Spanish.
-
Robustness of Fractional Flow Reserve for Lesion Assessment in Non-Infarct-Related Arteries of Patients With Myocardial Infarction.J Am Heart Assoc. 2019 May 7;8(9):e012456. doi: 10.1161/JAHA.119.012456. J Am Heart Assoc. 2019. PMID: 31014179 Free PMC article.
-
Functionally Complete Coronary Revascularisation in Patients Presenting with ST-elevation MI and Multivessel Coronary Artery Disease.Interv Cardiol. 2021 Jul 27;16:e24. doi: 10.15420/icr.2020.28. eCollection 2021 Apr. Interv Cardiol. 2021. PMID: 34400971 Free PMC article. Review.
References
-
- Neumann F‐J, Sousa‐Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, Byrne RA, Collet J‐P, Falk V, Head SJ, Jüni P, Kastrati A, Koller A, Kristensen SD, Niebauer J, Richter DJ, Seferovic PM, Sibbing D, Stefanini GG, Windecker S, Yadav R, Zembala MO; ESC Scientific Document Group . 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40:87–165. - PubMed
-
- Engstrøm T, Kelbæk H, Helqvist S, Høfsten DE, Kløvgaard L, Holmvang L, Jørgensen E, Pedersen F, Saunamäki K, Clemmensen P, De Backer O, Ravkilde J, Tilsted H‐H, Villadsen AB, Aarøe J, Jensen SE, Raungaard B, Køber L; DANAMI‐3—PRIMULTI Investigators . Complete revascularisation versus treatment of the culprit lesion only in patients with ST‐segment elevation myocardial infarction and multivessel disease (DANAMI‐3—PRIMULTI): an open‐label, randomised controlled trial. Lancet Lond Engl. 2015;386:665–671. - PubMed
-
- Smits PC, Abdel‐Wahab M, Neumann F‐J, Boxma‐de Klerk BM, Lunde K, Schotborgh CE, Piroth Z, Horak D, Wlodarczak A, Ong PJ, Hambrecht R, Angerås O, Richardt G, Omerovic E; Compare‐Acute Investigators . Fractional flow reserve‐guided multivessel angioplasty in myocardial infarction. N Engl J Med. 2017;376:1234–1244. - PubMed
-
- Wald DS, Morris JK, Wald NJ, Chase AJ, Edwards RJ, Hughes LO, Berry C, Oldroyd KG; PRAMI Investigators . Randomized trial of preventive angioplasty in myocardial infarction. N Engl J Med. 2013;369:1115–1123. - PubMed
-
- Gershlick AH, Khan JN, Kelly DJ, Greenwood JP, Sasikaran T, Curzen N, Blackman DJ, Dalby M, Fairbrother KL, Banya W, Wang D, Flather M, Hetherington SL, Kelion AD, Talwar S, Gunning M, Hall R, Swanton H, McCann GP. Randomized trial of complete versus lesion‐only revascularization in patients undergoing primary percutaneous coronary intervention for STEMI and multivessel disease: the CvLPRIT trial. J Am Coll Cardiol. 2015;65:963–972. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
