

Population-level mathematical modeling of antimicrobial resistance: a systematic review
- PMID: 31014341
- PMCID: PMC6480522
- DOI: 10.1186/s12916-019-1314-9
Population-level mathematical modeling of antimicrobial resistance: a systematic review
Abstract
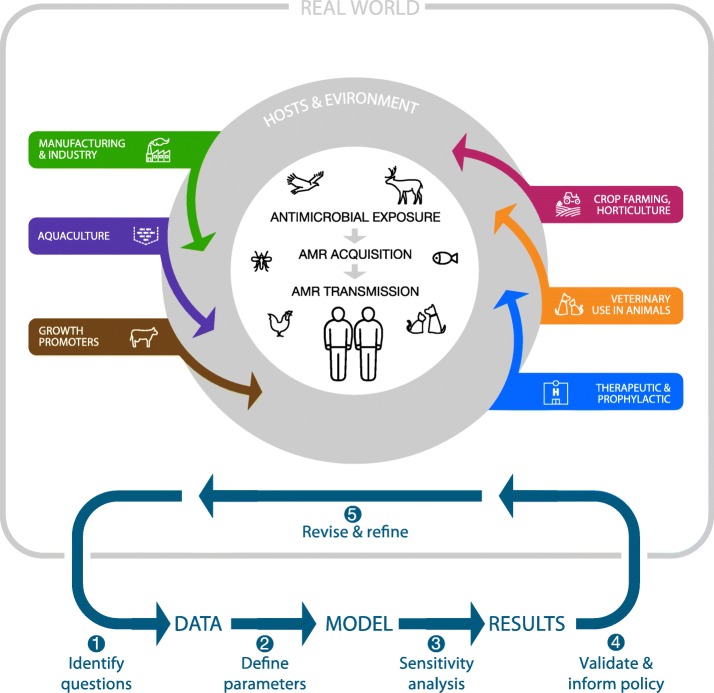
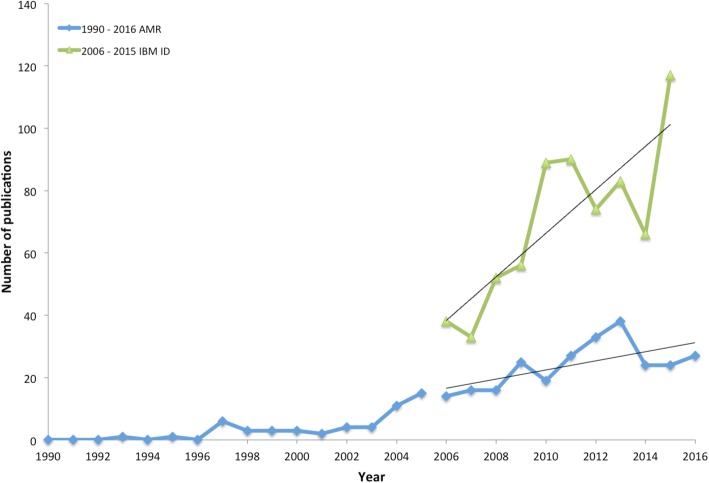
Background: Mathematical transmission models are increasingly used to guide public health interventions for infectious diseases, particularly in the context of emerging pathogens; however, the contribution of modeling to the growing issue of antimicrobial resistance (AMR) remains unclear. Here, we systematically evaluate publications on population-level transmission models of AMR over a recent period (2006-2016) to gauge the state of research and identify gaps warranting further work.
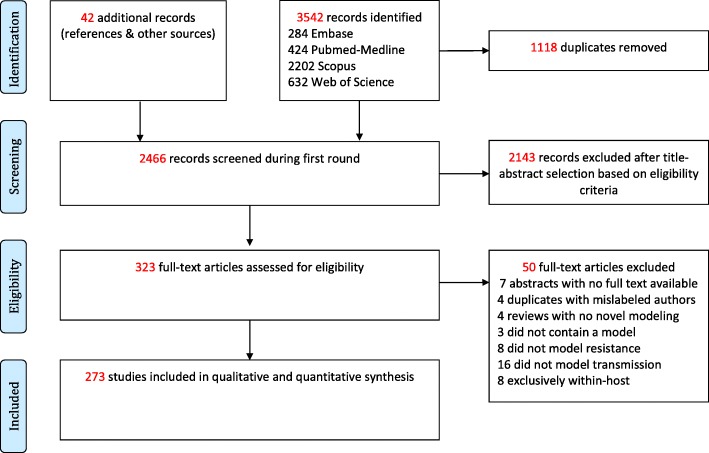
Methods: We performed a systematic literature search of relevant databases to identify transmission studies of AMR in viral, bacterial, and parasitic disease systems. We analyzed the temporal, geographic, and subject matter trends, described the predominant medical and behavioral interventions studied, and identified central findings relating to key pathogens.
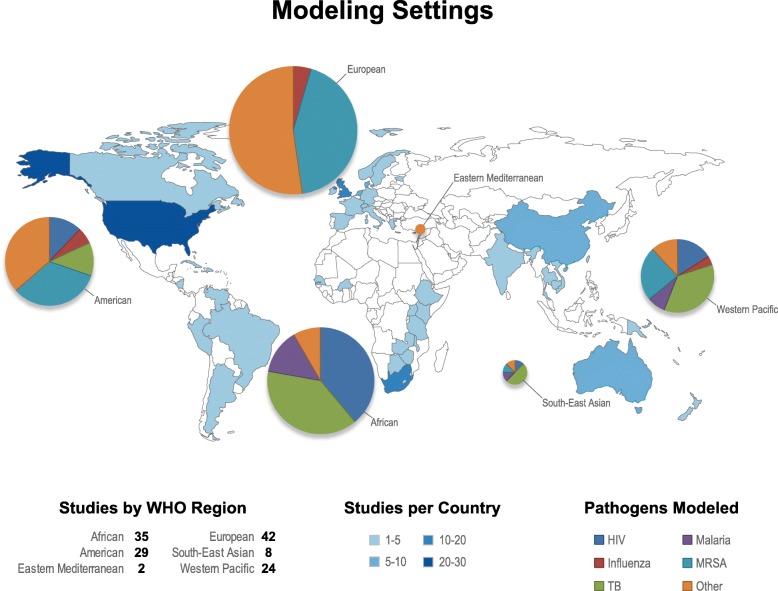
Results: We identified 273 modeling studies; the majority of which (> 70%) focused on 5 infectious diseases (human immunodeficiency virus (HIV), influenza virus, Plasmodium falciparum (malaria), Mycobacterium tuberculosis (TB), and methicillin-resistant Staphylococcus aureus (MRSA)). AMR studies of influenza and nosocomial pathogens were mainly set in industrialized nations, while HIV, TB, and malaria studies were heavily skewed towards developing countries. The majority of articles focused on AMR exclusively in humans (89%), either in community (58%) or healthcare (27%) settings. Model systems were largely compartmental (76%) and deterministic (66%). Only 43% of models were calibrated against epidemiological data, and few were validated against out-of-sample datasets (14%). The interventions considered were primarily the impact of different drug regimens, hygiene and infection control measures, screening, and diagnostics, while few studies addressed de novo resistance, vaccination strategies, economic, or behavioral changes to reduce antibiotic use in humans and animals.
Conclusions: The AMR modeling literature concentrates on disease systems where resistance has been long-established, while few studies pro-actively address recent rise in resistance in new pathogens or explore upstream strategies to reduce overall antibiotic consumption. Notable gaps include research on emerging resistance in Enterobacteriaceae and Neisseria gonorrhoeae; AMR transmission at the animal-human interface, particularly in agricultural and veterinary settings; transmission between hospitals and the community; the role of environmental factors in AMR transmission; and the potential of vaccines to combat AMR.
Keywords: Antimicrobial; Communicable diseases; Computational; Epidemiology; Mathematical; Models; Resistance; Transmission.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Global geographic trends in antimicrobial resistance: the role of international travel.J Travel Med. 2019 Dec 23;26(8):taz036. doi: 10.1093/jtm/taz036. J Travel Med. 2019. PMID: 31115466 Review.
-
Impact of the WHO Integrated Stewardship Policy on the Control of Methicillin-Resistant Staphyloccus aureus and Third-Generation Cephalosporin-Resistant Escherichia coli: Using a Mathematical Modeling Approach.Bull Math Biol. 2022 Aug 5;84(9):97. doi: 10.1007/s11538-022-01051-1. Bull Math Biol. 2022. PMID: 35931917
-
Modeling the transmission of antibiotic-resistant Enterobacterales in the community: A systematic review.Epidemics. 2024 Sep;48:100783. doi: 10.1016/j.epidem.2024.100783. Epub 2024 Jun 25. Epidemics. 2024. PMID: 38944024
-
Understanding the Impact of Interventions to Prevent Antimicrobial Resistant Infections in the Long-Term Care Facility: A Review and Practical Guide to Mathematical Modeling.Infect Control Hosp Epidemiol. 2017 Feb;38(2):216-225. doi: 10.1017/ice.2016.286. Epub 2016 Dec 19. Infect Control Hosp Epidemiol. 2017. PMID: 27989239 Review.
-
Antimicrobial use and antimicrobial resistance trends in Canada: 2014.Can Commun Dis Rep. 2016 Nov 3;42(11):227-231. doi: 10.14745/ccdr.v42i11a02. eCollection 2016 Nov 3. Can Commun Dis Rep. 2016. PMID: 29769991 Free PMC article.
Cited by
-
Bayesian Calibration to Address the Challenge of Antimicrobial Resistance: A Review.IEEE Access. 2024;12:100772-100791. doi: 10.1109/ACCESS.2024.3427410. IEEE Access. 2024. PMID: 39286062 Free PMC article.
-
Analyses of Extended-Spectrum-β-Lactamase, Metallo-β-Lactamase, and AmpC-β-Lactamase Producing Enterobacteriaceae from the Dairy Value Chain in India.Antibiotics (Basel). 2023 Sep 14;12(9):1449. doi: 10.3390/antibiotics12091449. Antibiotics (Basel). 2023. PMID: 37760745 Free PMC article.
-
Collateral impacts of pandemic COVID-19 drive the nosocomial spread of antibiotic resistance: A modelling study.PLoS Med. 2023 Jun 5;20(6):e1004240. doi: 10.1371/journal.pmed.1004240. eCollection 2023 Jun. PLoS Med. 2023. PMID: 37276186 Free PMC article.
-
Modelling the implementation of narrow versus broader spectrum antibiotics in the empiric treatment of E. coli bacteraemia.Sci Rep. 2024 Jul 23;14(1):16986. doi: 10.1038/s41598-024-66193-9. Sci Rep. 2024. PMID: 39043719 Free PMC article.
-
Antiviral polysaccharide and antiviral peptide delivering nanomaterials for prevention and treatment of SARS-CoV-2 caused COVID-19 and other viral diseases.J Control Release. 2023 Jun;358:476-497. doi: 10.1016/j.jconrel.2023.05.010. Epub 2023 May 14. J Control Release. 2023. PMID: 37164241 Free PMC article. Review.
References
-
- WHO . Antimicrobial resistance: global report on surveillance 2014. 2014. p. 257.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
