

Late immune consequences of combat trauma: a review of trauma-related immune dysfunction and potential therapies
- PMID: 31014397
- PMCID: PMC6480837
- DOI: 10.1186/s40779-019-0202-0
Late immune consequences of combat trauma: a review of trauma-related immune dysfunction and potential therapies
Abstract
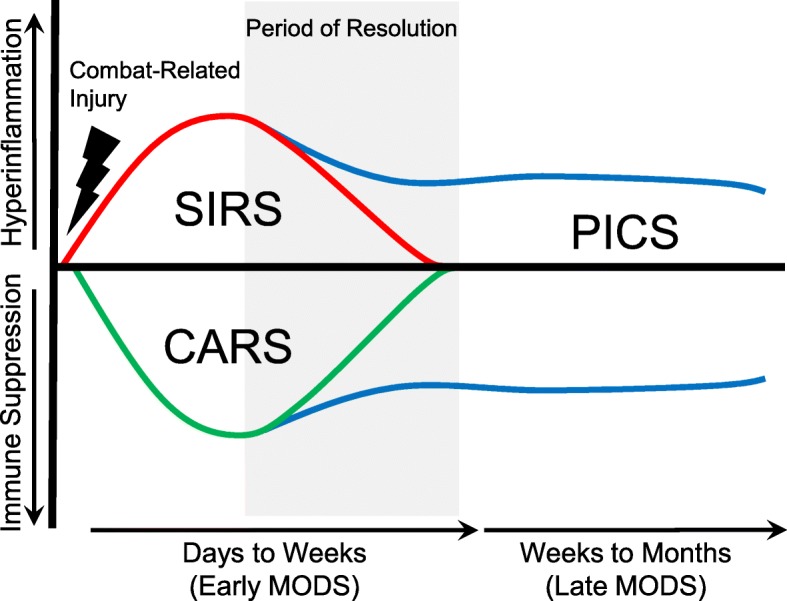
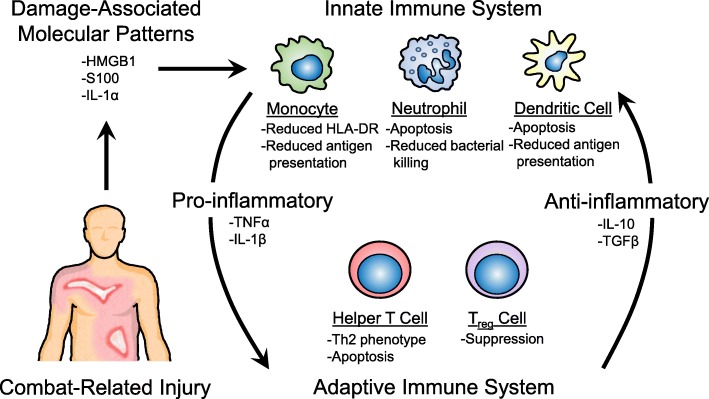
With improvements in personnel and vehicular body armor, robust casualty evacuation capabilities, and damage control resuscitation strategies, more combat casualties are surviving to reach higher levels of care throughout the casualty evacuation system. As such, medical centers are becoming more accustomed to managing the deleterious late consequences of combat trauma related to the dysregulation of the immune system. In this review, we aim to highlight these late consequences and identify areas for future research and therapeutic strategies. Trauma leads to the dysregulation of both the innate and adaptive immune responses, which places the injured at risk for several late consequences, including delayed wound healing, late onset sepsis and infection, multi-organ dysfunction syndrome, and acute respiratory distress syndrome, which are significant for their association with the increased morbidity and mortality of wounded personnel. The mechanisms by which these consequences develop are complex but include an imbalance of the immune system leading to robust inflammatory responses, triggered by the presence of damage-associated molecules and other immune-modifying agents following trauma. Treatment strategies to improve outcomes have been difficult to develop as the immunophenotype of injured personnel following trauma is variable, fluid and difficult to determine. As more information regarding the triggers that lead to immune dysfunction following trauma is elucidated, it may be possible to identify the immunophenotype of injured personnel and provide targeted treatments to reduce the late consequences of trauma, which are known to lead to significant morbidity and mortality.
Keywords: Compensatory anti-inflammatory response syndrome; Immune dysfunction; Persistent inflammation-immunosuppression and catabolism syndrome; Sepsis; Trauma.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Air Force, Navy, the Department of Defense or the U.S. Government (KBT, LTK).
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
