

Statins for primary prevention of cardiovascular disease: modelling guidelines and patient preferences based on an Irish cohort
- PMID: 31015226
- PMCID: PMC6532821
- DOI: 10.3399/bjgp19X702701
Statins for primary prevention of cardiovascular disease: modelling guidelines and patient preferences based on an Irish cohort
Abstract
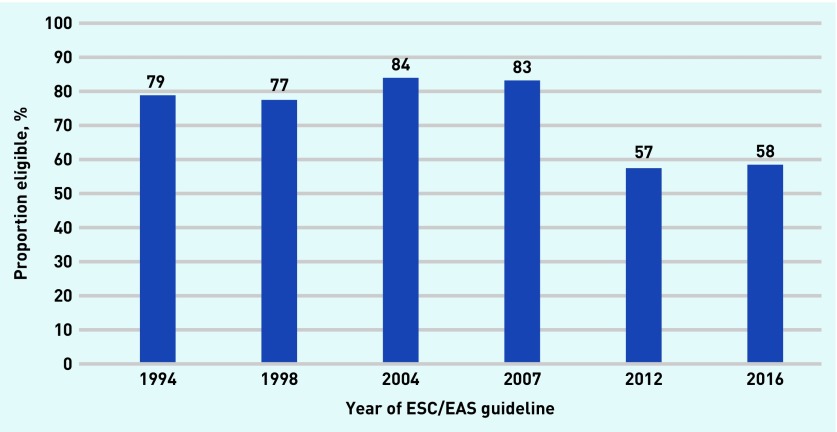
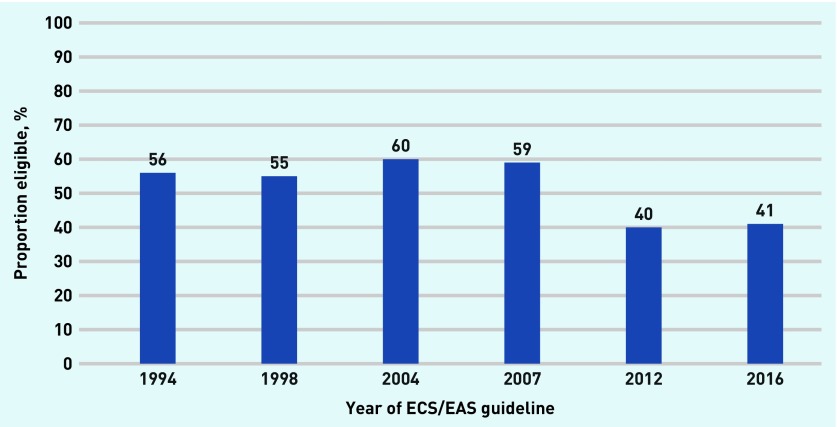
Background: Changes in clinical guidelines for primary prevention of cardiovascular disease (CVD) have widened eligibility for statin therapy.
Aim: To illustrate the potential impacts of changes in clinical guidelines.
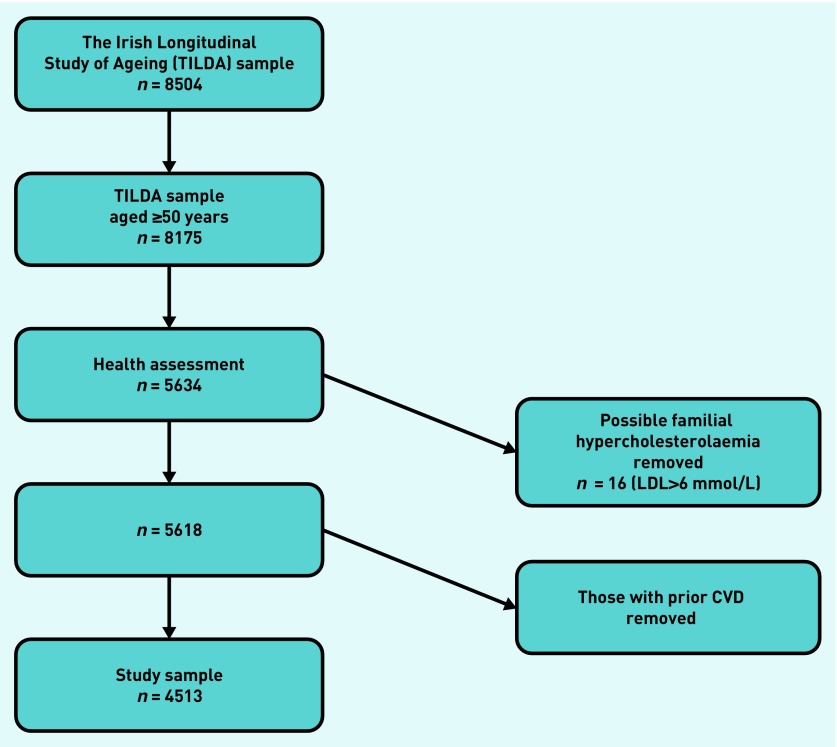
Design and setting: Modelling the impacts of seven consecutive European guidelines based on a cohort of people aged ≥50 years from the Irish Longitudinal Study on Ageing.
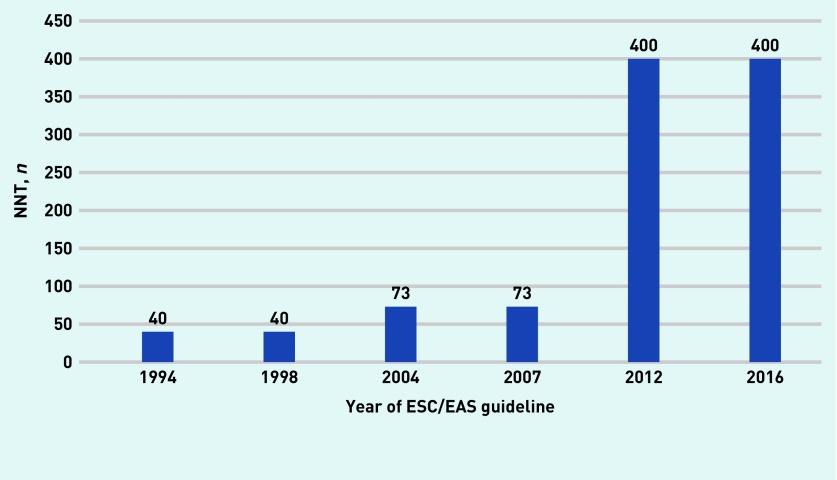
Method: The eligibility for statin therapy of a sample of people without a history of CVD was established, according to changing guideline recommendations and modelled associated potential costs. The authors calculated the numbers needed to treat (NNT) to prevent one major vascular event in patients at the lowest baseline risk for which each of the seven guidelines recommended treatment, and for those at low, medium, high, and very-high risk according to 2016 guidelines. These were compared with the NNT that patients reported as required to justify taking a daily medicine.
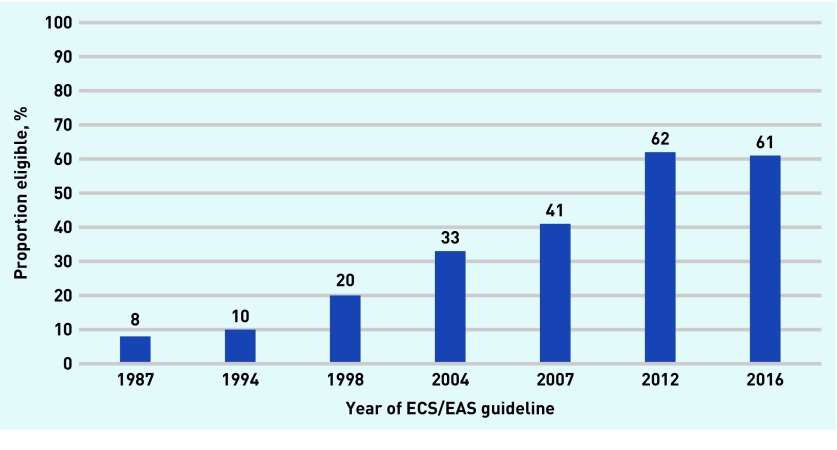
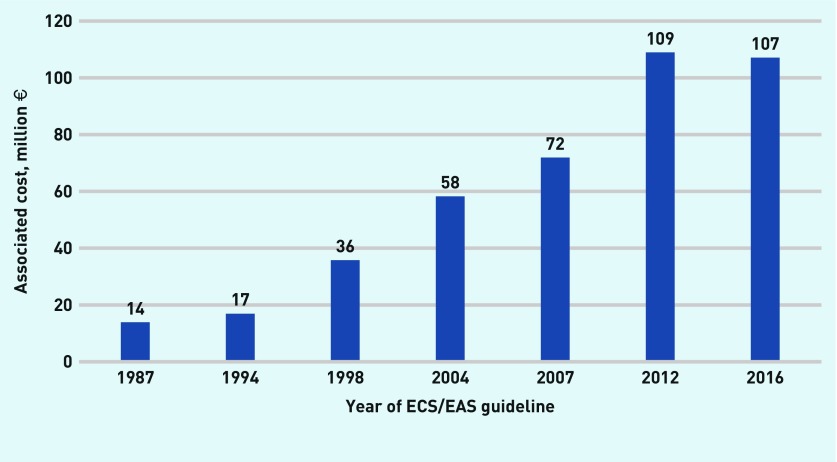
Results: The proportion of patients eligible for statins increased from approximately 8% in 1987 to 61% in 2016; associated costs rose from €13.9 million to €107.1 million per annum. The NNT for those at the lowest risk for which each guideline recommended treatment rose from 40 to 400. By 2016, the NNT for low-risk patients was 400 compared to ≤25 very-high risk patients. The proportion of patients eligible for statins achieving NNT levels that patients regarded as justified to taking a daily medicine fell as guidelines changed over time.
Conclusion: Increased eligibility for statin therapy impacts large proportions of the present population and healthcare budgets. Decisions to take and reimburse statins should be considered on the basis of expected cost-effectiveness and acceptability to patients.
Keywords: drug costs; guideline; hydroxymethylglutaryl-CoA reductase inhibitors, patient preference; primary prevention.
© British Journal of General Practice 2019.
Figures
References
-
- Feely J, McGettigan P, Kelly A. Growth in use of statins after trials is not targeted to most appropriate patients. Clin Pharmacol Ther. 2000;67(4):438–441. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical