

Molecular subtyping reveals immune alterations associated with progression of bronchial premalignant lesions
- PMID: 31015447
- PMCID: PMC6478943
- DOI: 10.1038/s41467-019-09834-2
Molecular subtyping reveals immune alterations associated with progression of bronchial premalignant lesions
Abstract
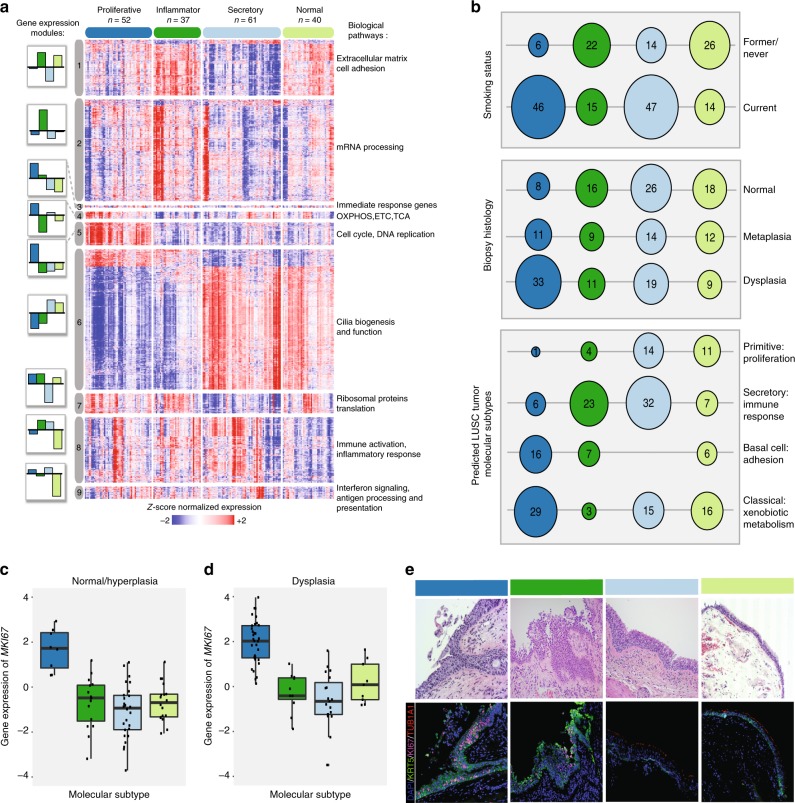
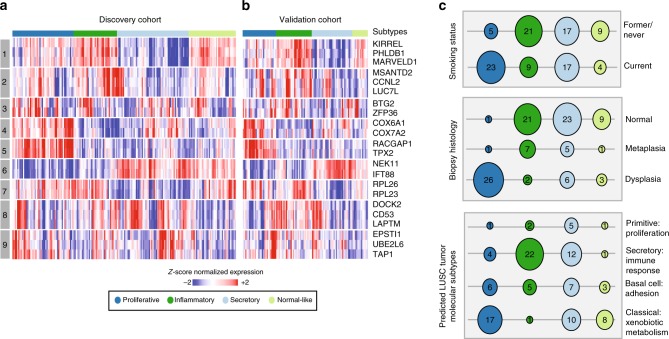
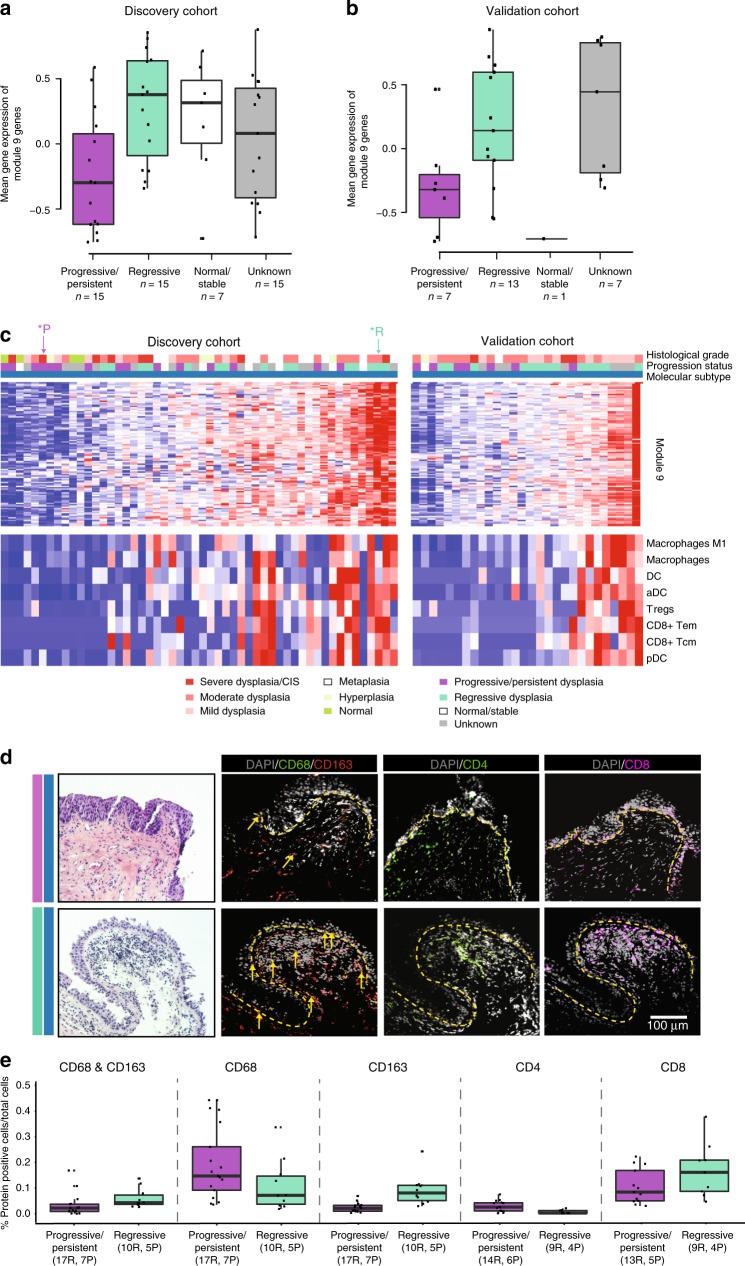
Bronchial premalignant lesions (PMLs) are precursors of lung squamous cell carcinoma, but have variable outcome, and we lack tools to identify and treat PMLs at risk for progression to cancer. Here we report the identification of four molecular subtypes of PMLs with distinct differences in epithelial and immune processes based on RNA-Seq profiling of endobronchial biopsies from high-risk smokers. The Proliferative subtype is enriched with bronchial dysplasia and exhibits up-regulation of metabolic and cell cycle pathways. A Proliferative subtype-associated gene signature identifies subjects with Proliferative PMLs from normal-appearing uninvolved large airway brushings with high specificity. In progressive/persistent Proliferative lesions expression of interferon signaling and antigen processing/presentation pathways decrease and immunofluorescence indicates a depletion of innate and adaptive immune cells compared with regressive lesions. Molecular biomarkers measured in PMLs or the uninvolved airway can enhance histopathological grading and suggest immunoprevention strategies for intercepting the progression of PMLs to lung cancer.
Conflict of interest statement
JEB, SAM, JDC, CP, JV, MER, MEL, and AES received commercial research grants from Janssen Pharmaceuticals. MEL is a consultant to Veracyte. AES, MS, CM, and CS are employed by Johnson and Johnson. SJP was employed by Johnson and Johnson during the study and is now employed by Covance. GD, KK, GL, SZ, HL, SSD, and SMD declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
