

Adenosine receptor agonism protects against NETosis and thrombosis in antiphospholipid syndrome
- PMID: 31015489
- PMCID: PMC6478874
- DOI: 10.1038/s41467-019-09801-x
Adenosine receptor agonism protects against NETosis and thrombosis in antiphospholipid syndrome
Abstract
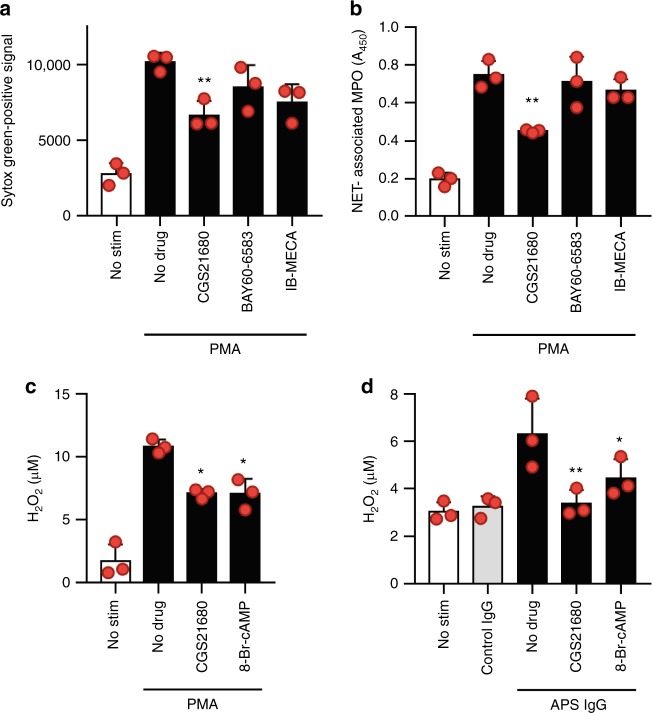
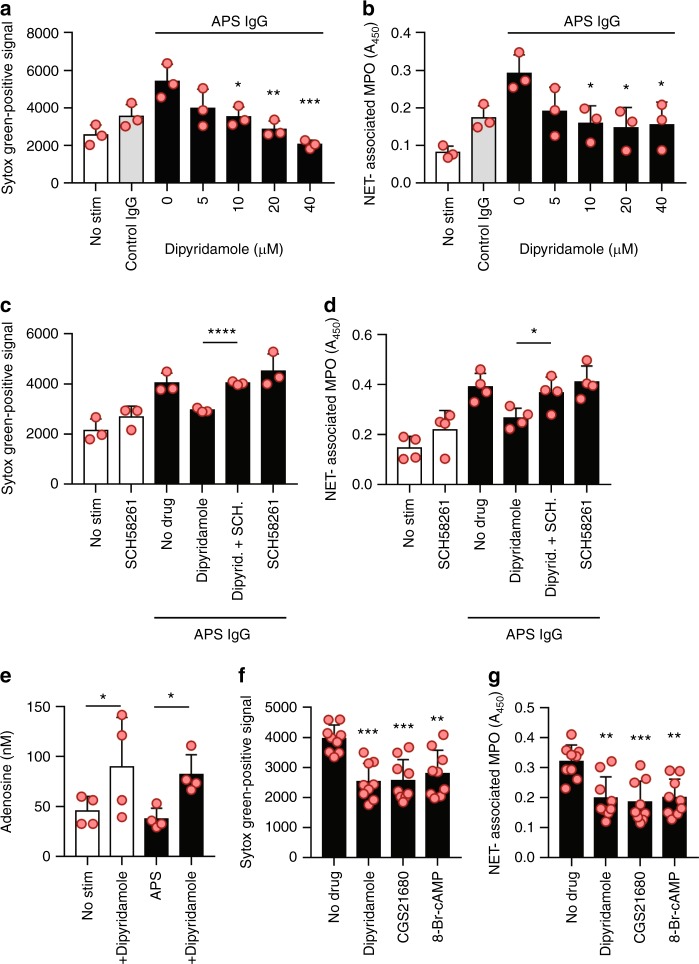
Potentiation of neutrophil extracellular trap (NET) release is one mechanism by which antiphospholipid antibodies (aPL Abs) effect thrombotic events in patients with antiphospholipid syndrome (APS). Surface adenosine receptors trigger cyclic AMP (cAMP) formation in neutrophils, and this mechanism has been proposed to regulate NETosis in some contexts. Here we report that selective agonism of the adenosine A2A receptor (CGS21680) suppresses aPL Ab-mediated NETosis in protein kinase A-dependent fashion. CGS21680 also reduces thrombosis in the inferior vena cavae of both control mice and mice administered aPL Abs. The antithrombotic medication dipyridamole is known to potentiate adenosine signaling by increasing extracellular concentrations of adenosine and interfering with the breakdown of cAMP. Like CGS21680, dipyridamole suppresses aPL Ab-mediated NETosis via the adenosine A2A receptor and mitigates venous thrombosis in mice. In summary, these data suggest an anti-inflammatory therapeutic paradigm in APS, which may extend to thrombotic disease in the general population.
Conflict of interest statement
The authors declare no competing interests.
Figures




Comment in
-
Preventing NETosis to reduce thrombosis.Nat Rev Rheumatol. 2019 Jun;15(6):317. doi: 10.1038/s41584-019-0234-6. Nat Rev Rheumatol. 2019. PMID: 31053832 No abstract available.
References
-
- Abreu MM, et al. The relevance of “non-criteria” clinical manifestations of antiphospholipid syndrome: 14th International Congress on Antiphospholipid Antibodies Technical Task Force Report on Antiphospholipid Syndrome Clinical Features. Autoimmun. Rev. 2015;14:401–414. doi: 10.1016/j.autrev.2015.01.002. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
