

Comparative Efficacy and Tolerability of Neoadjuvant Immunotherapy Regimens for Patients with HER2-Positive Breast Cancer: A Network Meta-Analysis
- PMID: 31015833
- PMCID: PMC6444249
- DOI: 10.1155/2019/3406972
Comparative Efficacy and Tolerability of Neoadjuvant Immunotherapy Regimens for Patients with HER2-Positive Breast Cancer: A Network Meta-Analysis
Abstract
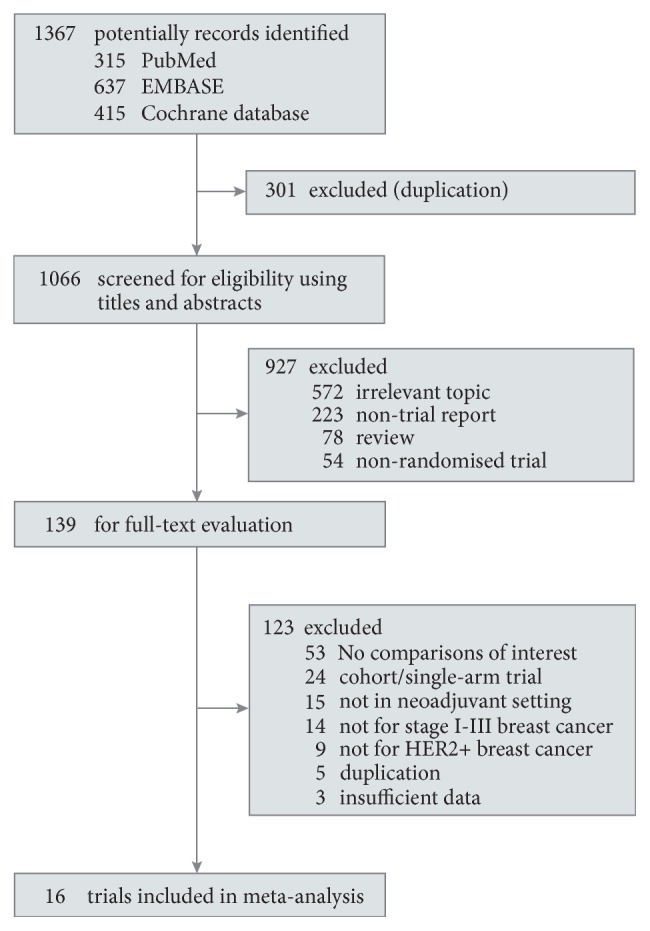
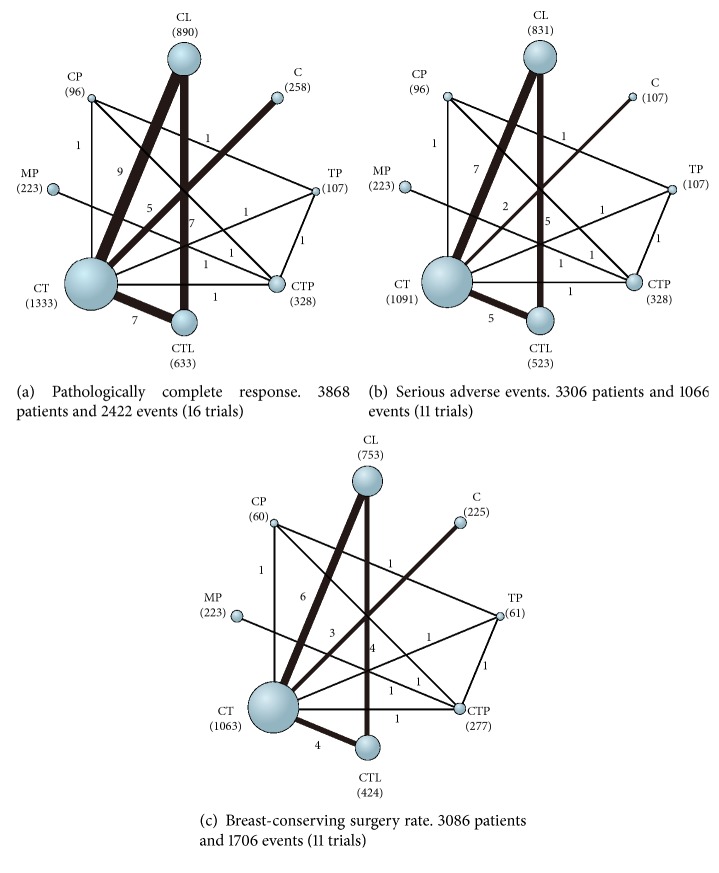
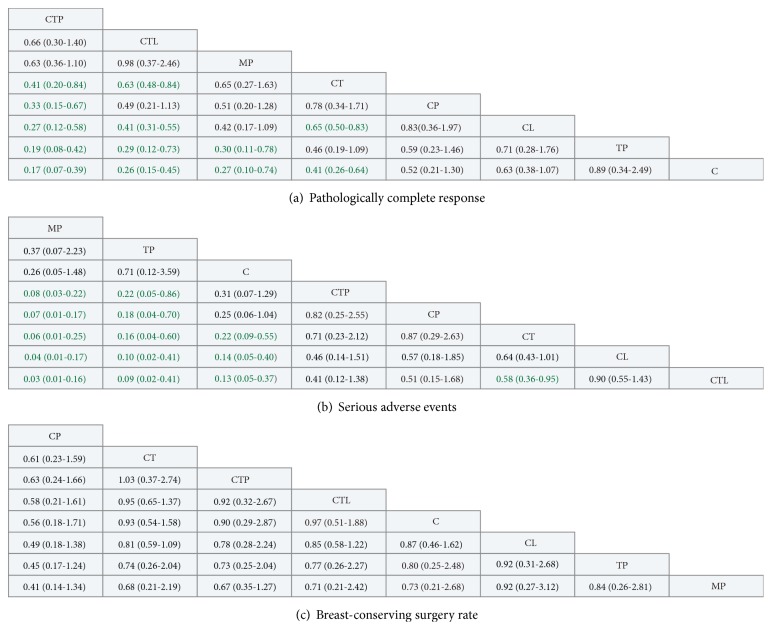
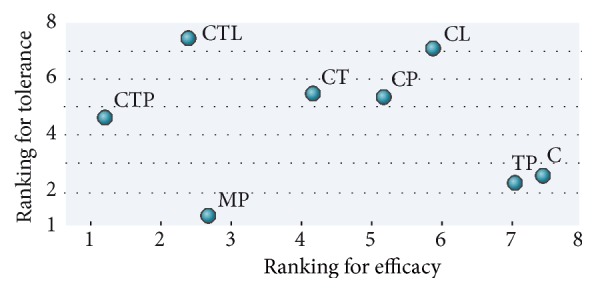
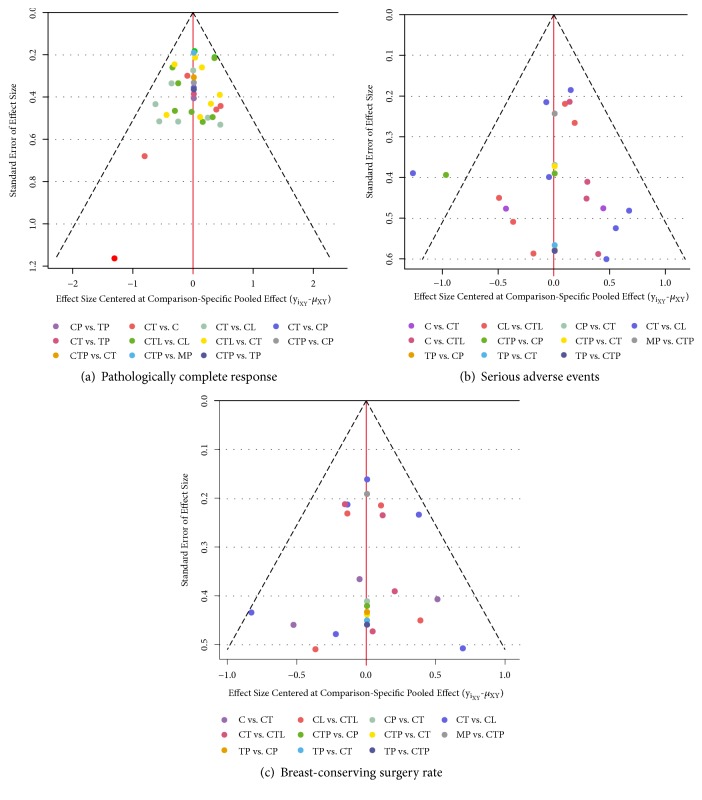
This network meta-analysis addresses the need for evidence-based best-practice treatment regimens for HER2-positive breast cancer. We compared the relative efficacy and tolerability of currently available HER2-positive neoadjuvant immunotherapy regimens based on systematic searches of available randomized controlled trials (RCTs) data. Based on intention-to-treat principle, pathological complete response (pCR), overall serious adverse events (SAEs), and breast-conserving surgery (BCS) rate were analyzed using random-effect, Bayesian network meta-analysis, and standard pairwise meta-analysis. 16 RCTs (3868 patients) were included. Analyzed treatment regimens were as follows: chemotherapy+trastuzumab+pertuzumab (CTP), trastuzumab emtansine+pertuzumab (MP), chemotherapy+trastuzumab (CT), chemotherapy+pertuzumab (CP), trastuzumab+pertuzumab (TP), chemotherapy+trastuzumab+lapatinib (CTL), and chemotherapy+lapatinib (CL), and chemotherapy (C) alone. We found that, for the chance of achieving pCR, CTP was ranked first (SUCRA: 97%), followed by CTL, MP, and CT (SUCRA: 80%, 75%, and 55%, resp.). MP provided the safest regimen (SUCRA: 97%), then TP, C, and TPC (SUCRA: 82%, 76%, and 47%, resp.). CTL proved the most toxic therapy (SUCRA: 7%). No significant difference between neoadjuvant regimens was identified for BCS. Hormone receptor status did not impact ORs for pCR in any regimen. In conclusion, our findings support CTP as the optimum neoadjuvant regimen for HER2-positive breast cancer, with the best pCR and acceptable toxicity compared with CT. MP provides a therapeutic option for patients with poor performance status.
Figures
References
-
- Zell J. A., Tsang W. Y., Taylor T. H., Mehta R. S., Anton-Culver H. Prognostic impact of human epidermal growth factor-like receptor 2 and hormone receptor status in inflammatory breast cancer (IBC): analysis of 2,014 IBC patient cases from the California Cancer Registry. Breast Cancer Research. 2009;11(1, article R9) - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
