

Syringobulbia in Patients with Chiari Malformation Type I: A Systematic Review
- PMID: 31016190
- PMCID: PMC6444244
- DOI: 10.1155/2019/4829102
Syringobulbia in Patients with Chiari Malformation Type I: A Systematic Review
Abstract
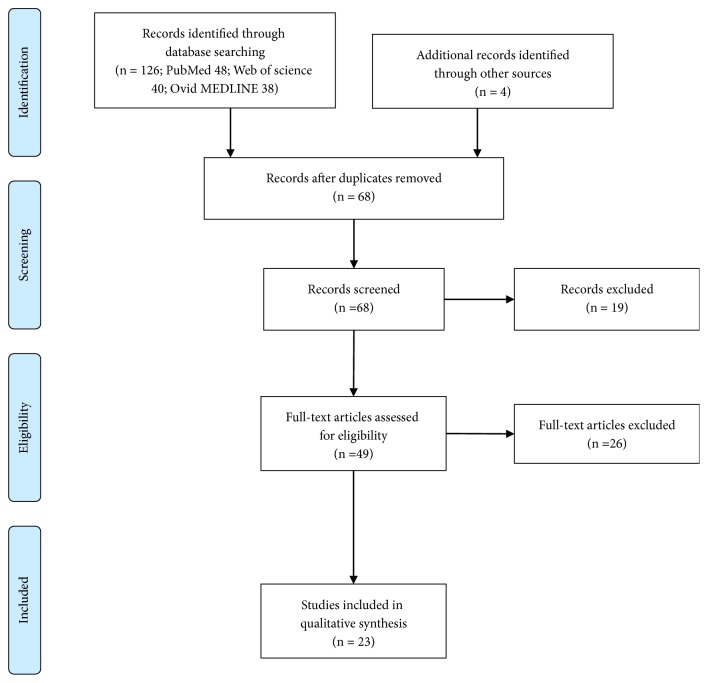
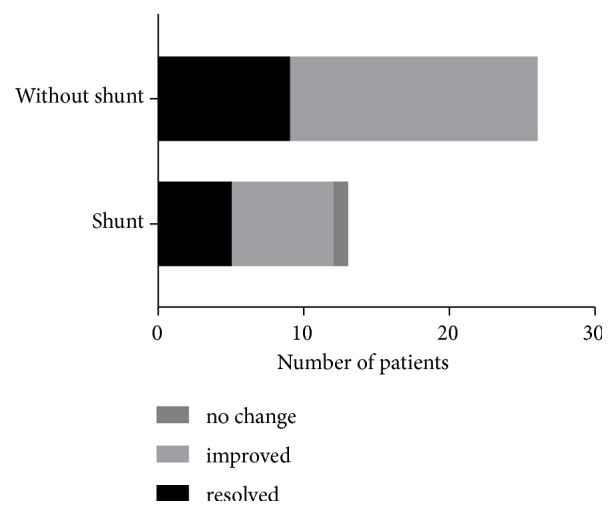
This study aimed to summarize the clinical features, diagnosis, and treatment of Chiari malformation type I- (CM-1-) associated syringobulbia. We performed a literature review of CM-1-associated syringobulbia in PubMed, Ovid MEDLINE, and Web of Science databases. Our concerns were the clinical features, radiologic presentations, treatment therapies, and prognoses of CM-1-associated syringobulbia. This review identified 23 articles with 53 cases. Symptoms included headache, neck pain, cranial nerve palsy, limb weakness/dysesthesia, Horner syndrome, ataxia, and respiratory disorders. The most frequently involved area was the medulla. Most of the patients also had syringomyelia. Surgical procedures performed included posterior fossa decompression, foramen magnum decompression, cervical laminectomy, duraplasty, and syringobulbic cavity shunt. Most patients experienced symptom alleviation or resolution postoperatively. A syringobulbic cavity shunt provided good results in refractory cases. Physicians should be aware of the possibility of syringobulbia in CM-1 patients, especially those with symptoms of sudden-onset brain-stem involvement. The diagnosis relies on the disorder's specific symptomatology and magnetic resonance imaging. Our review suggests that the initial therapy should be posterior fossa decomposition with or without duraplasty. In refractory cases, additional syringobulbic cavity shunt is the preferred option.
Figures
References
-
- Sharafuddin M. J. Syringomyelia extending to basal ganglia. Journal of Neurosurgery. 1990;73(4):p. 645. - PubMed
-
- Botelho R. V., Bittencourt L. R. A., Rotta J. M., Tufik S. Polysomnographic respiratory findings in patients with Arnold-Chiari type I malformation and basilar invagination, with or without syringomyelia: Preliminary report of a series of cases. Neurosurgical Review. 2000;23(3):151–155. doi: 10.1007/PL00011947. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
