

18F-FDG PET-CT versus MRI for detection of skeletal metastasis in Ewing sarcoma
- PMID: 31016339
- PMCID: PMC6776481
- DOI: 10.1007/s00256-019-03192-2
18F-FDG PET-CT versus MRI for detection of skeletal metastasis in Ewing sarcoma
Abstract
Objective: To determine the level of discrepancy between magnetic resonance imaging (MRI) and 18F-FDG PET-CT in detecting osseous metastases in patients with Ewing sarcoma.
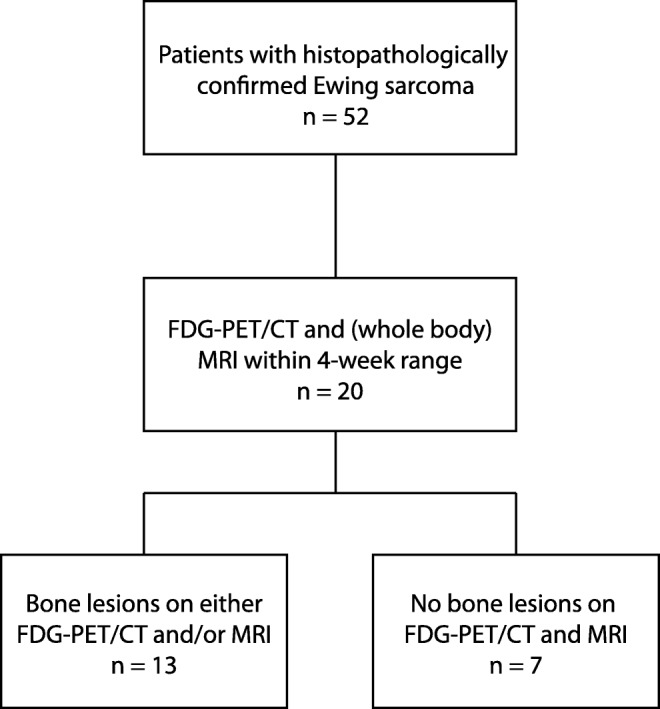
Methods: Twenty patients with histopathologically confirmed Ewing sarcoma between 2000 and 2017 who underwent 18F-FDG PET-CT and MRI within a 4-week range were included. Each imaging modality was evaluated by a separate observer. Reference diagnosis of each lesion was based on histopathology or consensus of an expert panel using all available data, including at least 6 months' follow-up. Sensitivity, specificity, and predictive values were determined. Osseous lesions were analyzed on a patient and a lesion basis. Factors possibly related to false-negative findings were evaluated using Pearson's Chi-squared or Fisher's exact test.
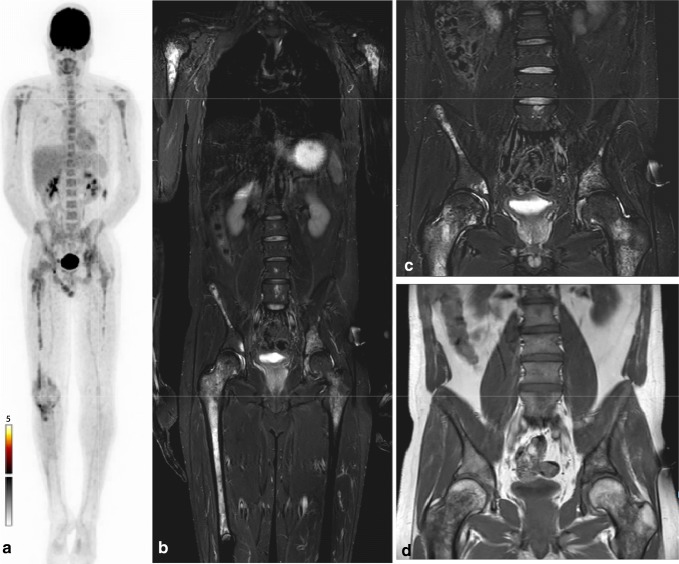
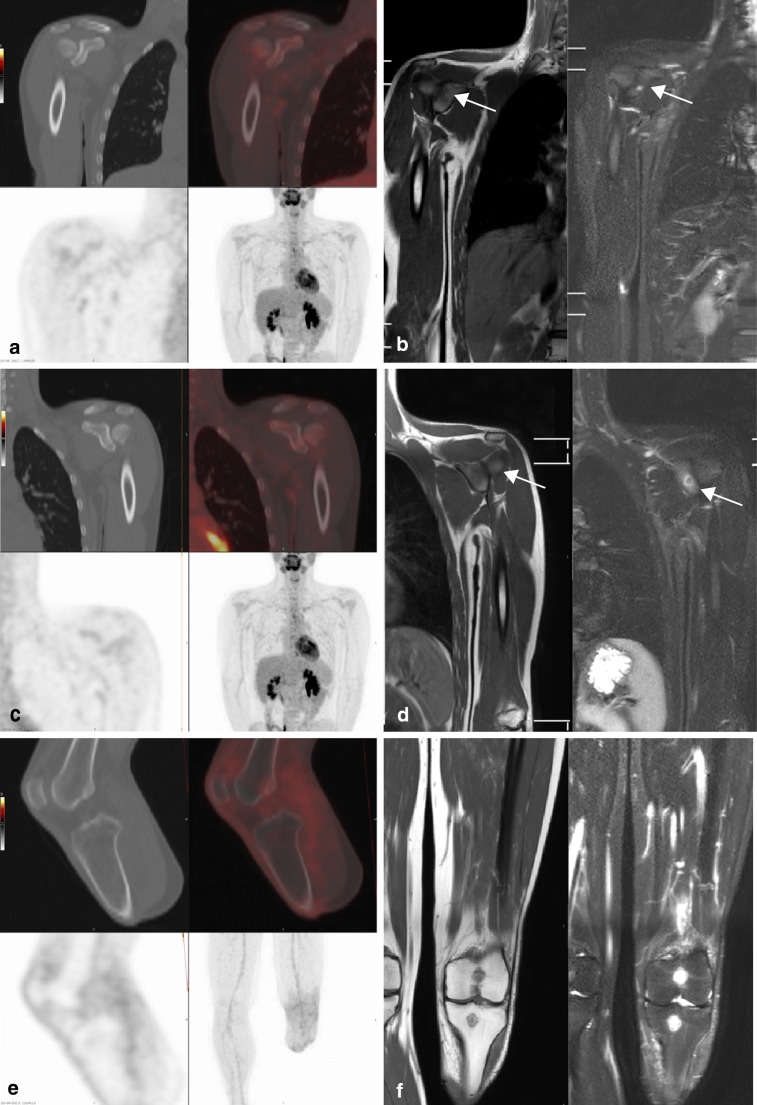
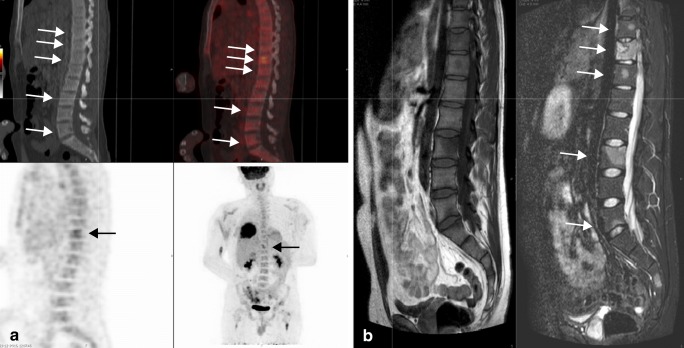
Results: A total of 112 osseous lesions were diagnosed in 13 patients, 107 malignant and 5 benign. Seven patients showed no metastases on either 18F-FDG PET-CT or MRI. Forty-one skeletal metastases (39%) detected with MRI did not show increased 18F-FDG uptake on 18F-FDG PET-CT (false-negative). Lesion-based sensitivities and specificities were 62% (95%CI 52-71%) and 100% (48-100%) for 18F-FDG PET-CT; and 99% (97-100%) and 100% (48-100%) for MRI respectively. Bone lesions were more likely to be false-negative on 18F-FDG PET-CT if hematopoietic bone marrow extension was widespread and active (p = 0.001), during or after (neo)-adjuvant treatment (p = 0.001) or when the lesion was smaller than 10 mm (p < 0.001).
Conclusion: Although no definite conclusions can be drawn from this small retrospective study, it shows that caution is needed when using 18F-FDG PET-CT for diagnosing skeletal metastases in Ewing sarcoma. Poor contrast between metastases and active hematopoietic bone marrow, chemotherapeutic treatment, and/or small size significantly decrease the diagnostic yield of 18F-FDG PET-CT, but not of MRI.
Keywords: Diagnosis; Ewing sarcoma; Magnetic resonance imaging; Osseous metastasis; Positron emission tomography with computerized tomography.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

Similar articles
-
What Is the Comparative Ability of 18F-FDG PET/CT, 99mTc-MDP Skeletal Scintigraphy, and Whole-body MRI as a Staging Investigation to Detect Skeletal Metastases in Patients with Osteosarcoma and Ewing Sarcoma?Clin Orthop Relat Res. 2021 Aug 1;479(8):1768-1779. doi: 10.1097/CORR.0000000000001681. Clin Orthop Relat Res. 2021. PMID: 33635285 Free PMC article.
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
Diagnostic performance of 18F-FDG PET/CT and whole-body diffusion-weighted imaging with background body suppression (DWIBS) in detection of lymph node and bone metastases from pediatric neuroblastoma.Ann Nucl Med. 2018 Jun;32(5):348-362. doi: 10.1007/s12149-018-1254-z. Epub 2018 Apr 17. Ann Nucl Med. 2018. PMID: 29667143 Free PMC article.
-
Post-treatment FDG PET/CT predicts progression-free survival in young patients with small round blue cell tumors: Ewing sarcoma and PNET.Eur J Radiol. 2020 Aug;129:109076. doi: 10.1016/j.ejrad.2020.109076. Epub 2020 May 16. Eur J Radiol. 2020. PMID: 32446127 Review.
-
The Utility of 18FDG PET/CT Versus Bone Scan for Identification of Bone Metastases in a Pediatric Sarcoma Population and a Review of the Literature.J Pediatr Hematol Oncol. 2021 Mar 1;43(2):52-58. doi: 10.1097/MPH.0000000000001917. J Pediatr Hematol Oncol. 2021. PMID: 32815877 Review.
Cited by
-
Ewing sarcoma with very late metastasis in the skull: a case report.J Med Case Rep. 2022 Nov 15;16(1):419. doi: 10.1186/s13256-022-03656-5. J Med Case Rep. 2022. PMID: 36376967 Free PMC article. Review.
-
Ewing sarcoma of the temporal bone with aneurysmal bone cyst-like changes: A rare case report with an unusual radiological presentation.Neuroradiol J. 2024 Oct;37(5):640-644. doi: 10.1177/19714009231212358. Epub 2023 Nov 3. Neuroradiol J. 2024. PMID: 37923348
-
Whole-Body MRI in Musculoskeletal Oncology: A Comprehensive Review with Recommendations.Radiol Imaging Cancer. 2023 May;5(3):e220107. doi: 10.1148/rycan.220107. Radiol Imaging Cancer. 2023. PMID: 37144975 Free PMC article. Review.
-
Applications of Artificial Intelligence for Pediatric Cancer Imaging.AJR Am J Roentgenol. 2024 Aug;223(2):e2431076. doi: 10.2214/AJR.24.31076. Epub 2024 May 23. AJR Am J Roentgenol. 2024. PMID: 38809123 Free PMC article. Review.
-
Total-Body PET Imaging of Musculoskeletal Disorders.PET Clin. 2021 Jan;16(1):99-117. doi: 10.1016/j.cpet.2020.09.012. PET Clin. 2021. PMID: 33218607 Free PMC article. Review.
References
-
- Fletcher CDM, Bridge JA, Hogendoorn PCW, Mertens F. WHO classification of tumours of soft tissue and bone. 4. Lyon: IARC; 2013.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
