

Evaluation of Renal Stone Comminution and Injury by Burst Wave Lithotripsy in a Pig Model
- PMID: 31016998
- PMCID: PMC6798804
- DOI: 10.1089/end.2018.0886
Evaluation of Renal Stone Comminution and Injury by Burst Wave Lithotripsy in a Pig Model
Abstract
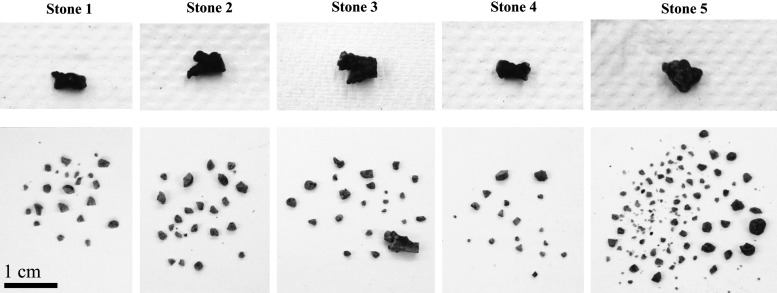
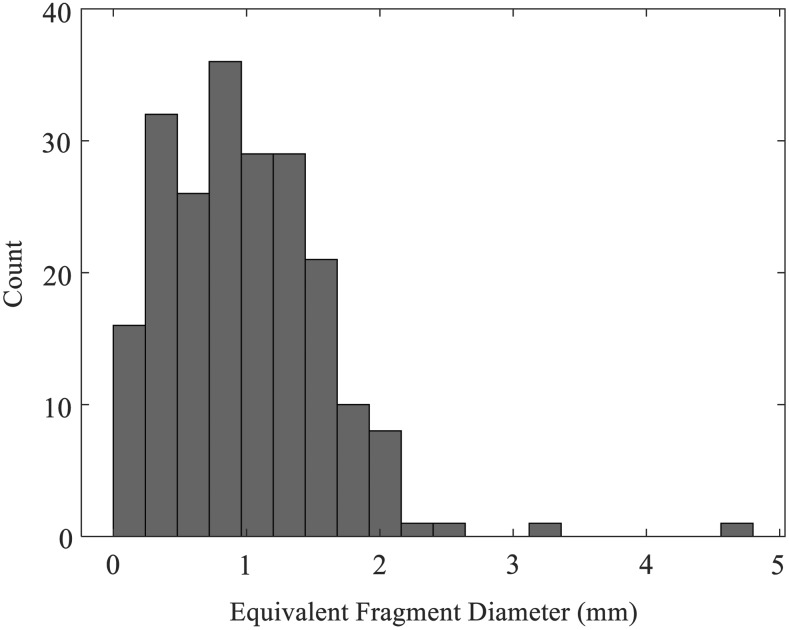
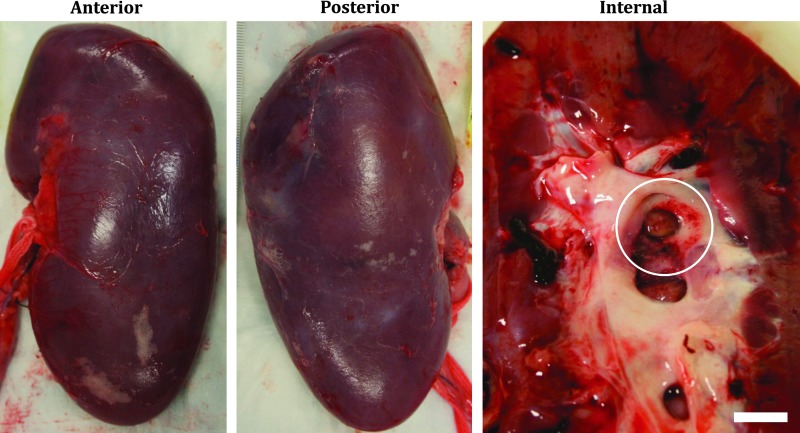
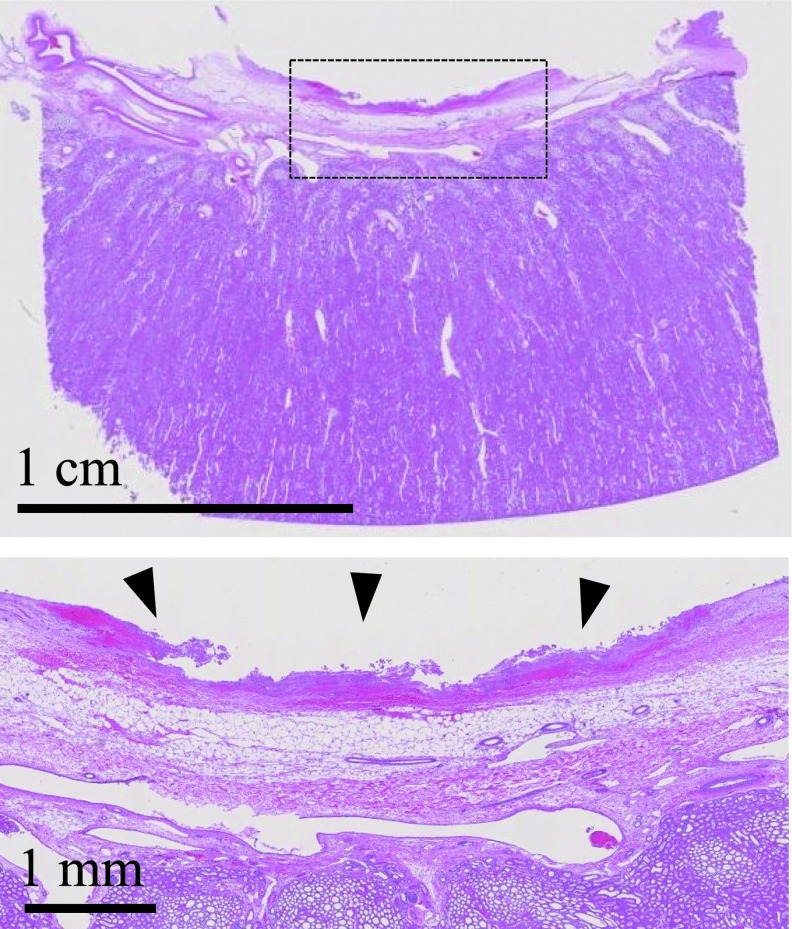
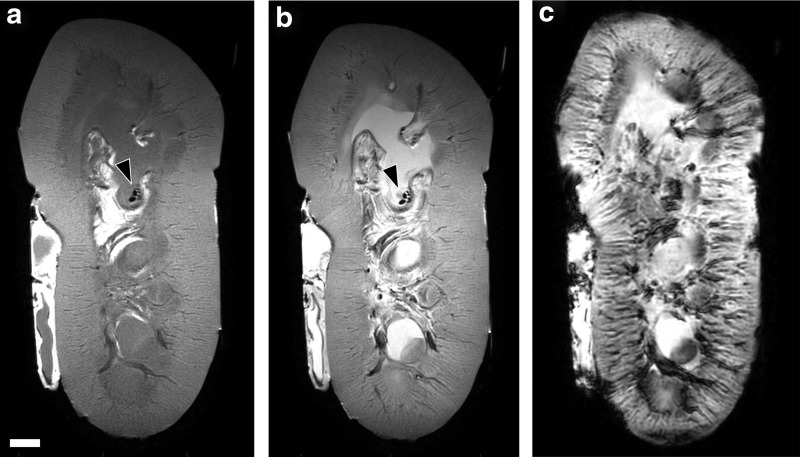
Introduction: Burst wave lithotripsy is an experimental technology to noninvasively fragment kidney stones with focused bursts of ultrasound (US). This study evaluated the safety and effectiveness of specific lithotripsy parameters in a porcine model of nephrolithiasis. Methods: A 6- to 7-mm human kidney stone was surgically implanted in each kidney of three pigs. A burst wave lithotripsy US transducer with an inline US imager was coupled to the flank and the lithotripter focus was aligned with the stone. Each stone was exposed to burst wave lithotripsy at 6.5 to 7 MPa focal pressure for 30 minutes under real-time image guidance. After treatment, the kidneys were removed for gross, histologic, and MRI assessment. Stone fragments were retrieved from the kidney to determine the mass comminuted to pieces <2 mm. Results: On average, 87% of the stone mass was reduced to fragments <2 mm. In three of five treatments, stones were completely comminuted to <2-mm fragments. In two of five treatments, stones were partially disintegrated, but larger fragments remained. One stone was not treated because no suitable acoustic window was identified. No injury was detected through gross, histologic, or MRI examination in the parenchymal tissue, although petechial damage and surface erosion were identified on the urothelium of the collecting system limited to the area around the stone. Conclusion: Burst wave lithotripsy can consistently produce stone fragments small enough to spontaneously pass by transcutaneous administration of US pulses. The data suggest that such exposures produce minimal injury to the kidney and urinary tract.
Keywords: burst wave lithotripsy; nephrolithiasis; renal injury; shock wave lithotripsy.
Conflict of interest statement
A.D.M., B.W.C., M.R.B., and M.D.S. have equity in and consulting agreements with SonoMotion, Inc., which has licensed technology related to this work from the University of Washington.
Figures
Comment in
-
Editorial Comment on: Evaluation of Renal Stone Comminution and Injury by Burst Wave Lithotripsy in a Pig Model by Maxwell et al. (From: Maxwell AD, Wang Y-N, Kreider W, et al. J Endourol 2019;33:787-792; DOI: 10.1089/end.2018.0886).J Endourol. 2019 Oct;33(10):793. doi: 10.1089/end.2019.0454. Epub 2019 Jul 31. J Endourol. 2019. PMID: 31266359 Free PMC article. No abstract available.
Similar articles
-
Detection and Evaluation of Renal Injury in Burst Wave Lithotripsy Using Ultrasound and Magnetic Resonance Imaging.J Endourol. 2017 Aug;31(8):786-792. doi: 10.1089/end.2017.0202. Epub 2017 Jun 16. J Endourol. 2017. PMID: 28521550 Free PMC article.
-
Fragmentation of urinary calculi in vitro by burst wave lithotripsy.J Urol. 2015 Jan;193(1):338-44. doi: 10.1016/j.juro.2014.08.009. Epub 2014 Aug 9. J Urol. 2015. PMID: 25111910 Free PMC article.
-
Comparison of tissue injury from focused ultrasonic propulsion of kidney stones versus extracorporeal shock wave lithotripsy.J Urol. 2014 Jan;191(1):235-41. doi: 10.1016/j.juro.2013.07.087. Epub 2013 Aug 2. J Urol. 2014. PMID: 23917165 Free PMC article.
-
Focused Ultrasound and Lithotripsy.Adv Exp Med Biol. 2016;880:113-29. doi: 10.1007/978-3-319-22536-4_7. Adv Exp Med Biol. 2016. PMID: 26486335 Review.
-
Burst wave lithotripsy and acoustic manipulation of stones.Curr Opin Urol. 2020 Mar;30(2):149-156. doi: 10.1097/MOU.0000000000000727. Curr Opin Urol. 2020. PMID: 31905177 Free PMC article. Review.
Cited by
-
Percutaneous nephrolithotomy in new versus those patients with previous history of Extracorporeal Shock Wave Lithotripsy on ipsilateral side.Pak J Med Sci. 2022 Mar-Apr;38(4Part-II):833-837. doi: 10.12669/pjms.38.4.5116. Pak J Med Sci. 2022. PMID: 35634635 Free PMC article.
-
An investigation of elastic waves producing stone fracture in burst wave lithotripsy.J Acoust Soc Am. 2020 Mar;147(3):1607. doi: 10.1121/10.0000847. J Acoust Soc Am. 2020. PMID: 32237849 Free PMC article.
-
High-frequency shock wave lithotripsy: stone comminution and evaluation of renal parenchyma injury in a porcine ex-vivo model.World J Urol. 2023 Jul;41(7):1929-1934. doi: 10.1007/s00345-023-04441-9. Epub 2023 Jun 7. World J Urol. 2023. PMID: 37284842 Free PMC article.
-
Agarose as a Tissue Mimic for the Porcine Heart, Kidney, and Liver: Measurements and a Springpot Model.Bioengineering (Basel). 2024 Jun 8;11(6):589. doi: 10.3390/bioengineering11060589. Bioengineering (Basel). 2024. PMID: 38927825 Free PMC article.
-
Proof-of-concept for a novel nanotechnology-based treatment for urolithiasis.Urolithiasis. 2024 Apr 6;52(1):60. doi: 10.1007/s00240-024-01564-5. Urolithiasis. 2024. PMID: 38581591 Free PMC article.
References
-
- Cleveland RO, McAteer JA. Physics of shock-wave lithotripsy. In: Arthur D. Smith MD, Gopal H. Badlani MD, Glenn M. Preminger MD, Louis R. Kavoussi MD. Smith's Textbook of Endourology. Hoboken, NJ: Wiley-Blackwell, 2012, pp. 527–558
-
- Bailey MR, Pishchalnikov YA, Sapozhnikov OA, et al. . Cavitation detection during shock-wave lithotripsy. Ultrasound Med Biol 2005;31:1245. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
