

Silent Brain Infarcts Following Cardiac Procedures: A Systematic Review and Meta-Analysis
- PMID: 31017035
- PMCID: PMC6512106
- DOI: 10.1161/JAHA.118.010920
Silent Brain Infarcts Following Cardiac Procedures: A Systematic Review and Meta-Analysis
Abstract
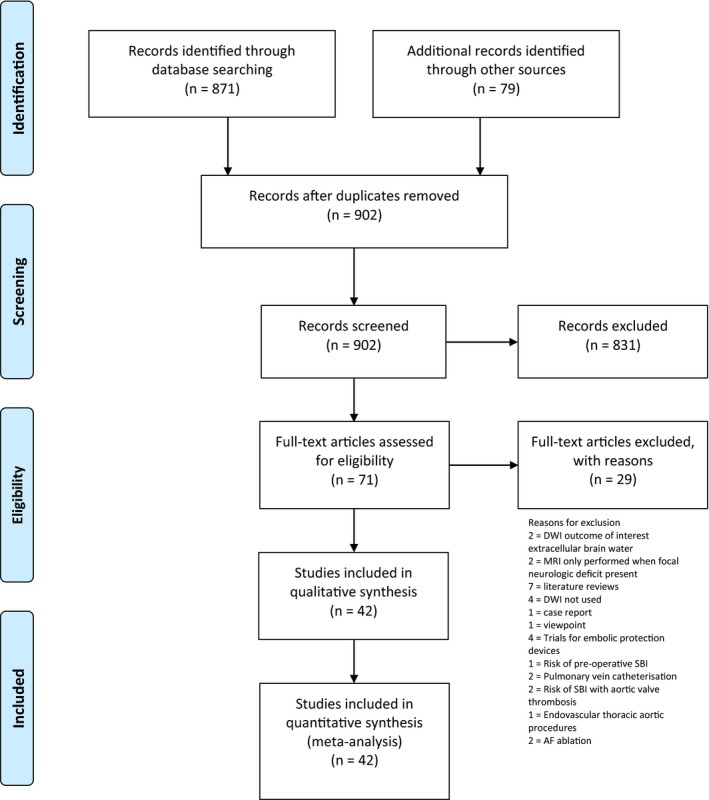
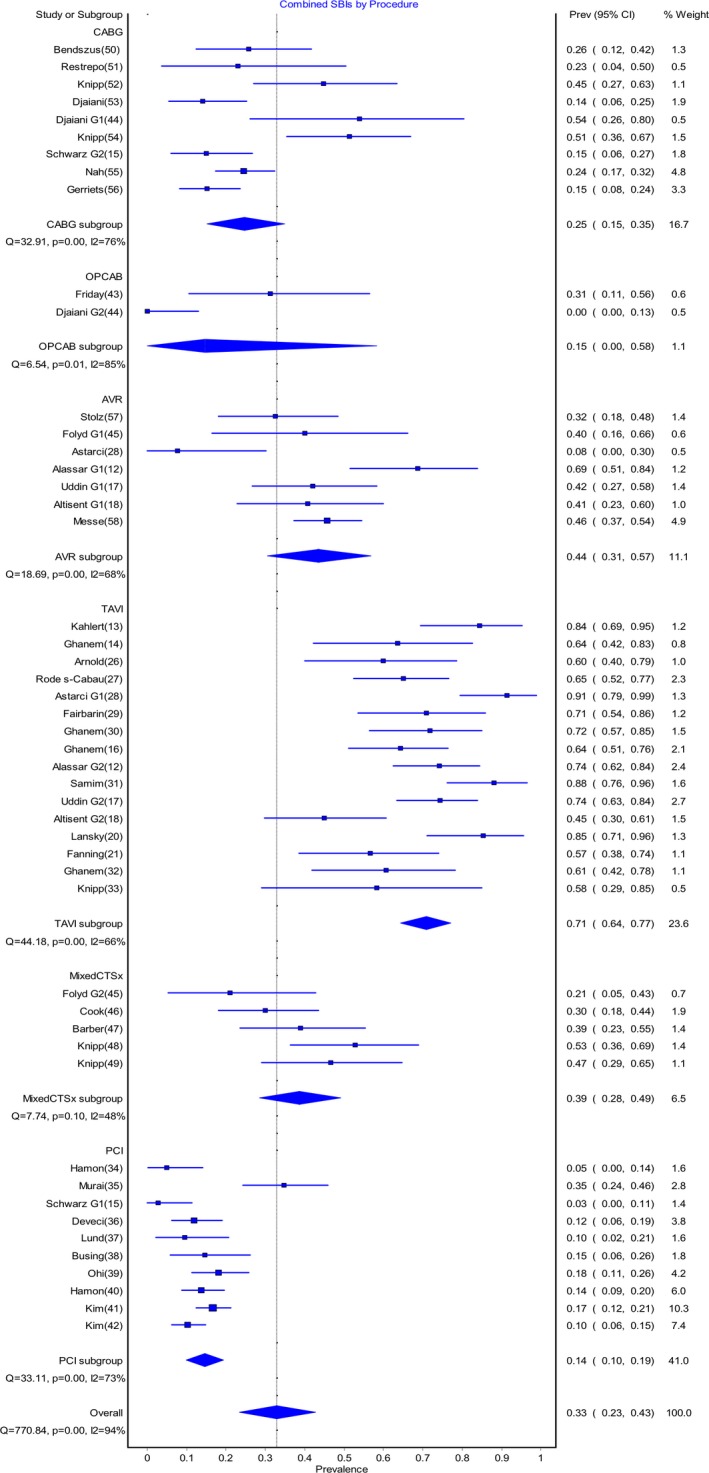
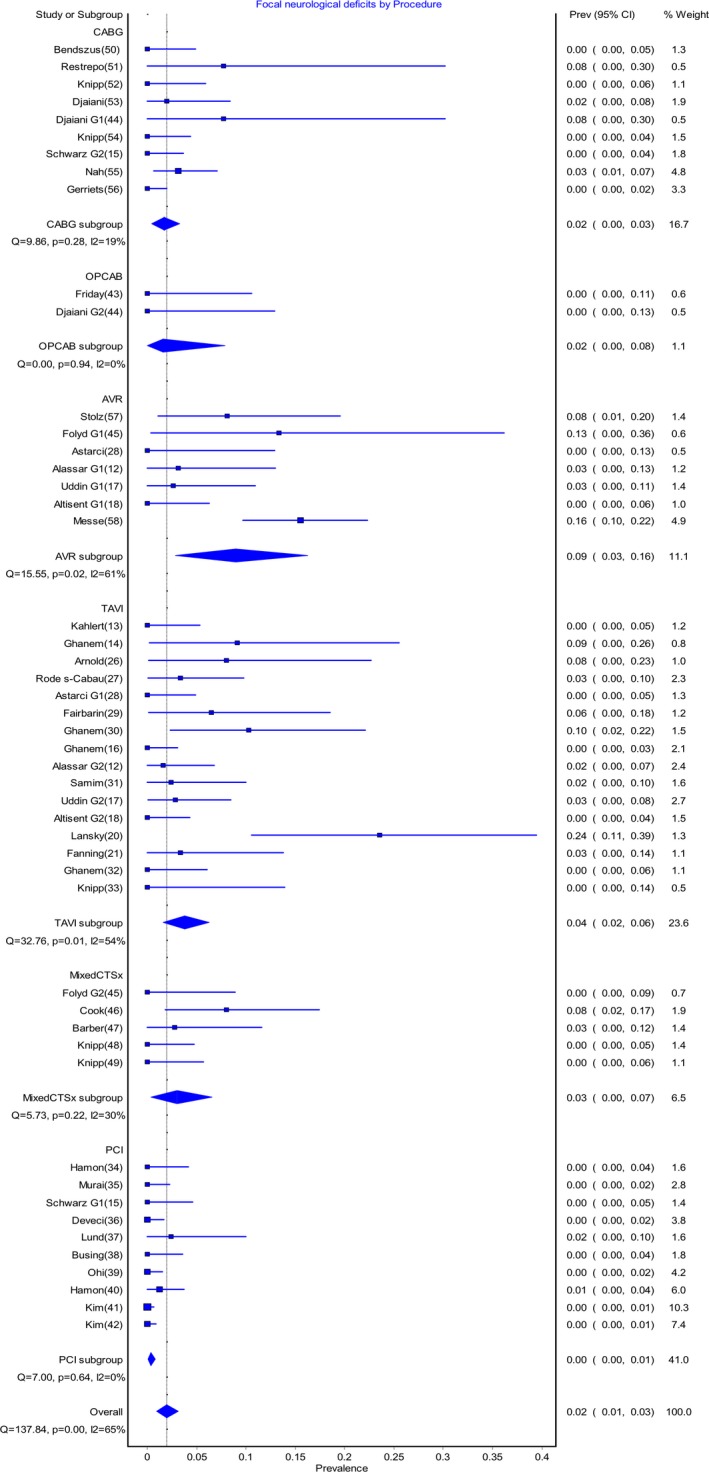
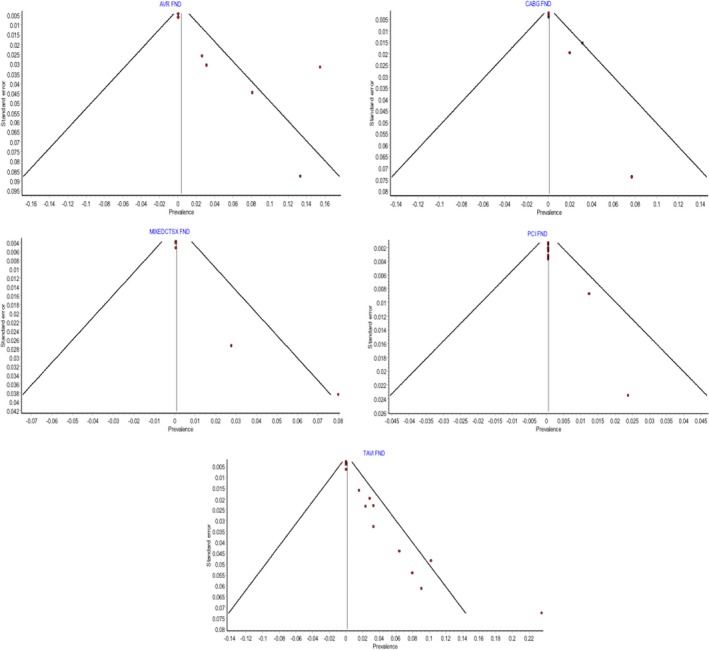
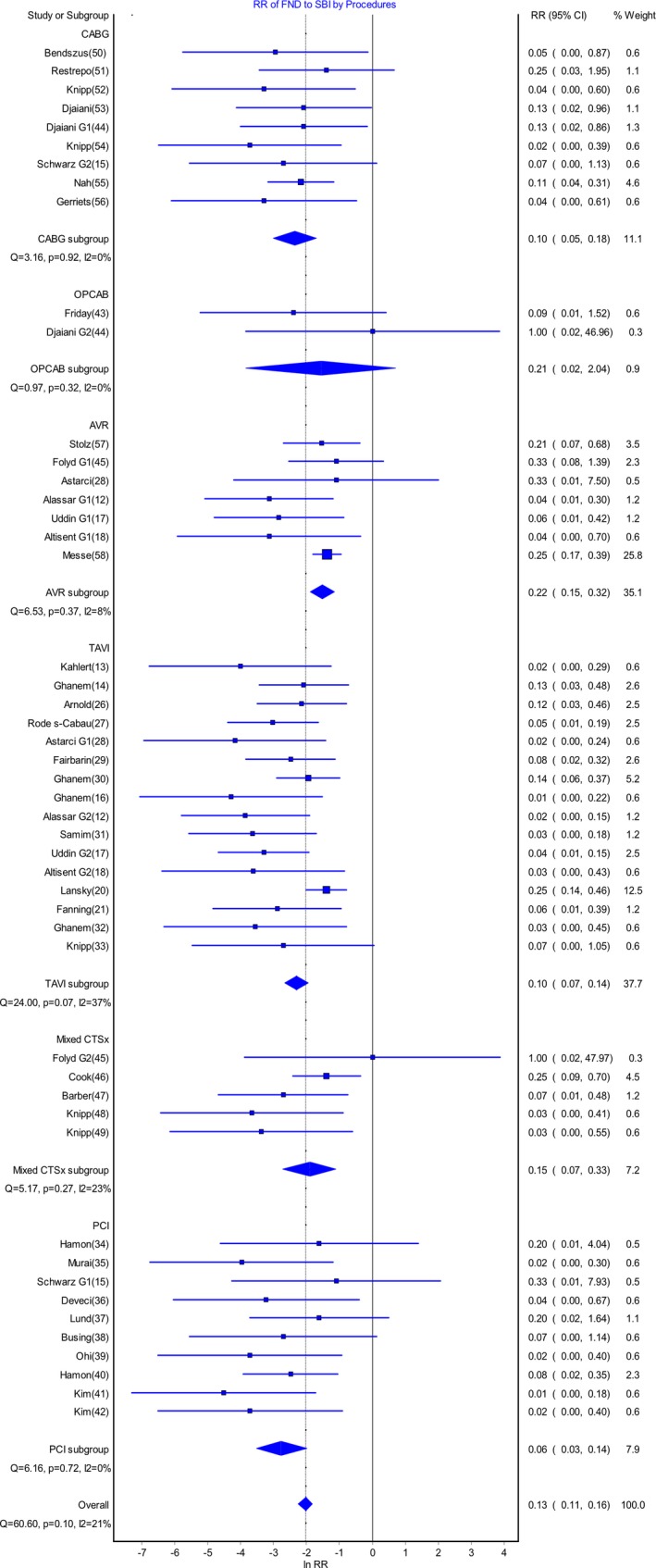
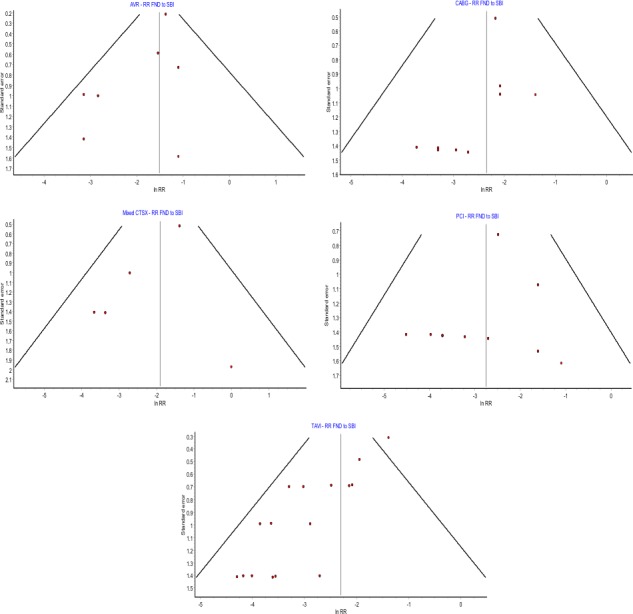
Background Silent brain infarcts ( SBI ) are increasingly being recognized as an important complication of cardiac procedures as well as a potential surrogate marker for studies on brain injury. The extent of subclinical brain injury is poorly defined. Methods and Results We conducted a systematic review and meta-analysis utilizing studies of SBI s and focal neurologic deficits following cardiac procedures. Our final analysis included 42 studies with 49 separate intervention groups for a total of 2632 patients. The prevalence of SBI s following transcatheter aortic valve implantation was 0.71 (95% CI 0.64-0.77); following aortic valve replacement 0.44 (95% CI 0.31-0.57); in a mixed cardiothoracic surgery group 0.39 (95% CI 0.28-0.49); coronary artery bypass graft 0.25 (95% CI 0.15-0.35); percutaneous coronary intervention 0.14 (95% CI 0.10-0.19); and off-pump coronary artery bypass 0.14 (0.00-0.58). The risk ratio of focal neurologic deficits to SBI in aortic valve replacement was 0.22 (95% CI 0.15-0.32); in off-pump coronary artery bypass 0.21 (95% CI 0.02-2.04); with mixed cardiothoracic surgery 0.15 (95% CI 0.07-0.33); coronary artery bypass graft 0.10 (95% CI 0.05-0.18); transcatheter aortic valve implantation 0.10 (95% CI 0.07-0.14); and percutaneous coronary intervention 0.06 (95% CI 0.03-0.14). The mean number of SBI s per patient was significantly higher in the transcatheter aortic valve implantation group (4.58 ± 2.09) compared with both the aortic valve replacement group (2.16 ± 1.62, P=0.03) and the percutaneous coronary intervention group (1.88 ± 1.02, P=0.03). Conclusions SBI s are a very common complication following cardiac procedures, particularly those involving the aortic valve. The high frequency of SBI s compared with strokes highlights the importance of recording this surrogate measure in cardiac interventional studies. We suggest that further work is required to standardize reporting in order to facilitate the use of SBI s as a routine outcome measure.
Keywords: cardiac surgery; magnetic resonance imaging; silent brain infarction; transapical aortic valve implantation.
Figures
References
-
- Edelman JJ, Yan TD, Bannon PG, Wilson MK, Vallely MP. Coronary artery bypass grafting with and without manipulation of the ascending aorta–a meta‐analysis. Heart Lung Circ. 2011;20:318–324. - PubMed
-
- Indraratna P, Tian DH, Yan TD, Doyle MP, Cao C. Transcatheter aortic valve implantation versus surgical aortic valve replacement: a meta‐analysis of randomized controlled trials. Int J Cardiol. 2016;224:382–387. - PubMed
-
- Miller DC, Blackstone EH, Mack MJ, Svensson LG, Kodali SK, Kapadia S, Rajeswaran J, Anderson WN, Moses JW, Tuzcu EM, Webb JG, Leon MB, Smith CR; PARTNER Trial Investigators and Patients, PARTNER Stroke Substudy Writing Group and Executive Committee . Transcatheter (TAVR) versus surgical (AVR) aortic valve replacement: occurrence, hazard, risk factors, and consequences of neurologic events in the PARTNER trial. J Thorac Cardiovasc Surg. 2012;143:832–843.e13 - PubMed
-
- Burdette JH, Ricci PE, Petitti N, Elster AD. Cerebral infarction: time course of signal intensity changes on diffusion‐weighted MR images. AJR Am J Roentgenol. 1998;171:791–795. - PubMed
-
- Provenzale JM, Sorensen AG. Diffusion‐weighted MR imaging in acute stroke: theoretic considerations and clinical applications. AJR Am J Roentgenol. 1999;173:1459–1467. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
