

Prostate cancer dose-response, fractionation sensitivity and repopulation parameters evaluation from 25 international radiotherapy outcome data sets
- PMID: 31017457
- PMCID: PMC6592096
- DOI: 10.1259/bjr.20180823
Prostate cancer dose-response, fractionation sensitivity and repopulation parameters evaluation from 25 international radiotherapy outcome data sets
Abstract
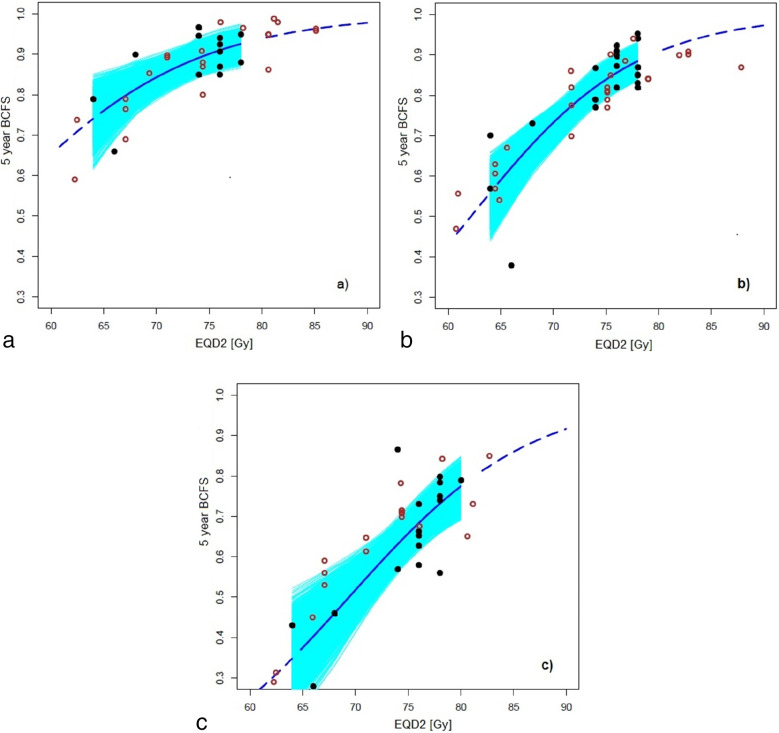
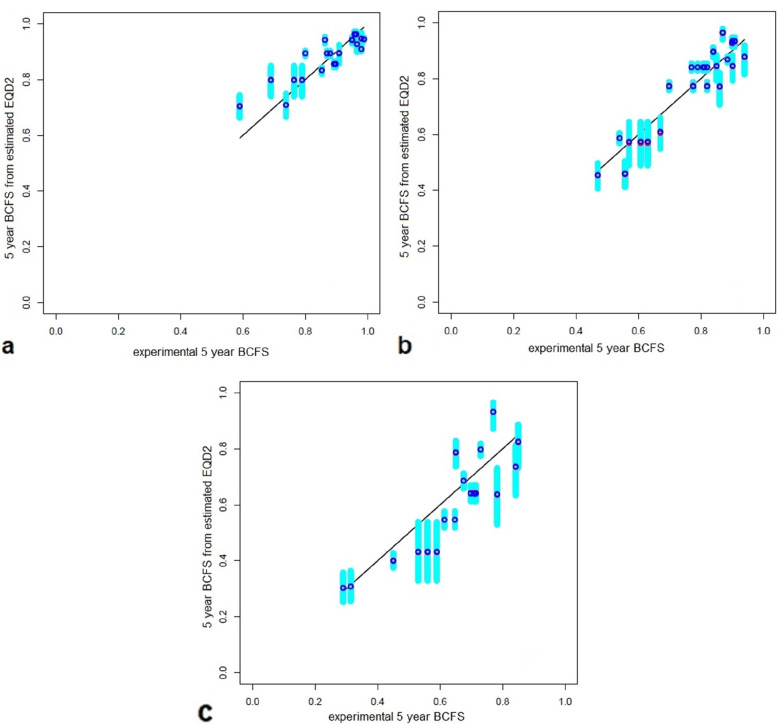
Objective: This study was undertaken to model the biochemical free survival at 5 years and to evaluate the parameters defining dose-response curve, dose-fractionation radiosensitivity and repopulation.
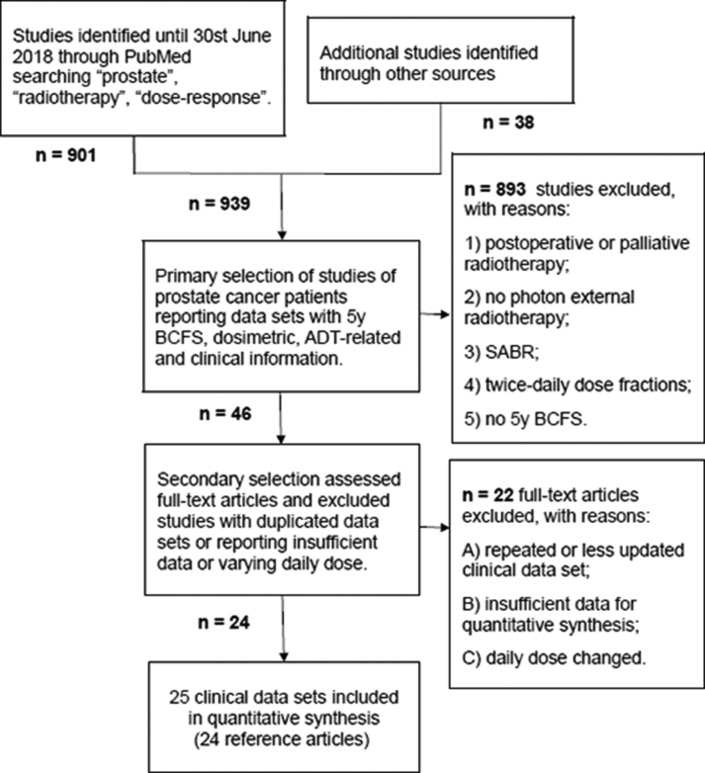
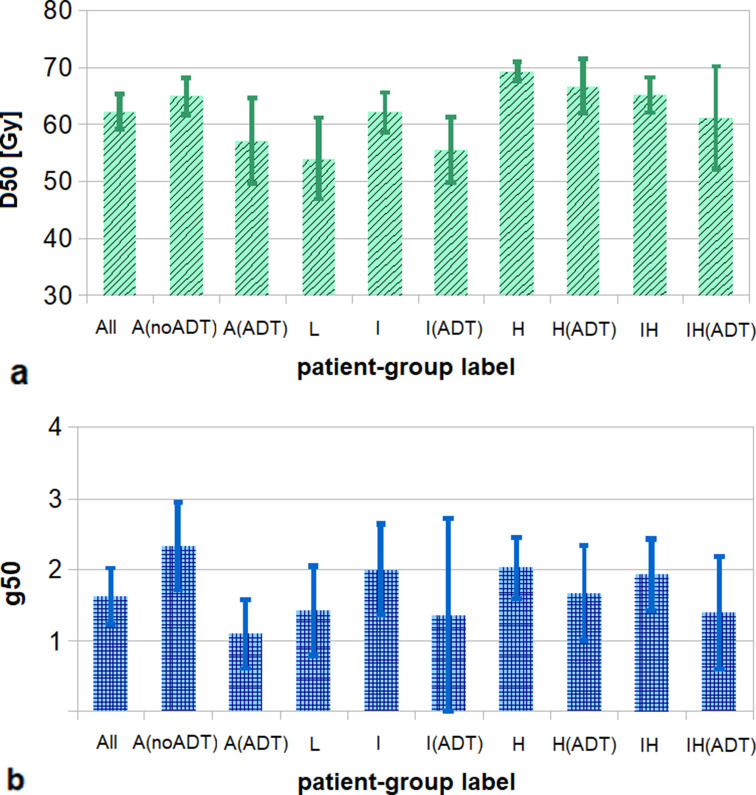
Methods: It was carried out a literature search on Pubmed to retrieve data sets of patients treated with external beam radiation therapy of 1.8-4.0 Gy per fraction and overall treatment time of 3 to 10 weeks. 10 groups were identified, based on risk class and androgen deprivation therapy (ADT). Dose-response curve D50 (dose at 50% probability of control) and g50 (steepness), α/β (dose-fractionation radiosensitivity), and repopulation parameters, dprolif and Tprolif , were calculated. Bootstrap-based cross-validation was performed and median and 95% CI (confidence interval) were evaluated.
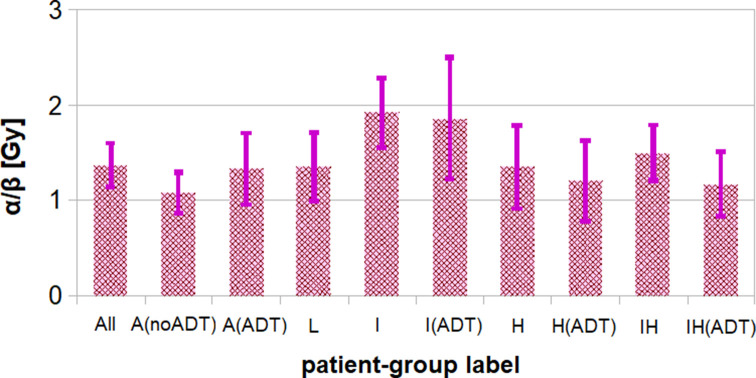
Results: 25 data sets, including 20,310 patients, were considered. The median (95% CI) D50 and g50 values were 62 (CI 53 - 66) Gy and 1.6 (0.8 - 2.4). ADT patients showed lower values of D50 and g50 (57 ± 5 Gy and 1.1 ± 0.4) compared to no-ADT patients (65 ± 2 Gy and 2.3 ± 0.6), with p < 0.0001 and p = 0.002. If we did not consider any dependence on overall treatment time, the median (95% CI) value of α/β was 1.4 (1.0 - 1.9) Gy with p < 0.0001 for all patients. The median values of dproli f and Tprolif were 0.0 to 0.3 Gy/d and 18-40 days.
Conclusion: Dose-response curve resulted dependent on risk class and ADT, with higher steepness for no-ADT patients. Low values of dose-fractionation radiosensitivity were found, supporting the use of moderate hypofractionated radiotherapy in each risk class. A limited dependence on repopulation was observed.
Advances in knowledge: Prostate cancer response to moderate hypofractionated radiotherapy was reliably quantified considering risk class and androgen deprivation therapy.
Figures
Similar articles
-
Prostate cancer tumour control probability modelling for external beam radiotherapy based on multi-parametric MRI-GTV definition.Radiat Oncol. 2020 Oct 20;15(1):242. doi: 10.1186/s13014-020-01683-4. Radiat Oncol. 2020. PMID: 33081804 Free PMC article.
-
Dose-fractionation sensitivity of prostate cancer deduced from radiotherapy outcomes of 5,969 patients in seven international institutional datasets: α/β = 1.4 (0.9-2.2) Gy.Int J Radiat Oncol Biol Phys. 2012 Jan 1;82(1):e17-24. doi: 10.1016/j.ijrobp.2010.10.075. Epub 2011 Feb 15. Int J Radiat Oncol Biol Phys. 2012. PMID: 21324610
-
Excellent results from high dose rate brachytherapy and external beam for prostate cancer are not improved by androgen deprivation.Am J Clin Oncol. 2009 Aug;32(4):342-7. doi: 10.1097/COC.0b013e31818cd277. Am J Clin Oncol. 2009. PMID: 19398902
-
Dose Response and Fractionation Sensitivity of Prostate Cancer After External Beam Radiation Therapy: A Meta-analysis of Randomized Trials.Int J Radiat Oncol Biol Phys. 2018 Mar 15;100(4):858-865. doi: 10.1016/j.ijrobp.2017.12.011. Epub 2017 Dec 15. Int J Radiat Oncol Biol Phys. 2018. PMID: 29485063
-
Hypofractionation for clinically localized prostate cancer.Cochrane Database Syst Rev. 2019 Sep 3;9(9):CD011462. doi: 10.1002/14651858.CD011462.pub2. Cochrane Database Syst Rev. 2019. PMID: 31476800 Free PMC article.
Cited by
-
Radiobiologically derived biphasic fractionation schemes to overcome the effects of tumour hypoxia.Br J Radiol. 2020 Aug;93(1112):20190250. doi: 10.1259/bjr.20190250. Epub 2020 Jun 2. Br J Radiol. 2020. PMID: 32462907 Free PMC article.
-
Normofractionated and moderately hypofractionated proton therapy: comparison of acute toxicity and early quality of life outcomes.Front Oncol. 2022 Aug 16;12:962697. doi: 10.3389/fonc.2022.962697. eCollection 2022. Front Oncol. 2022. PMID: 36052240 Free PMC article.
-
Generation of Radioresistant Prostate Cancer Cells.Methods Mol Biol. 2023;2645:129-138. doi: 10.1007/978-1-0716-3056-3_5. Methods Mol Biol. 2023. PMID: 37202614
-
Treatment Interruptions During Stereotactic Body Radiotherapy for Prostate Cancer.Front Oncol. 2022 Jan 19;11:796496. doi: 10.3389/fonc.2021.796496. eCollection 2021. Front Oncol. 2022. PMID: 35127506 Free PMC article.
References
-
- Duchesne GM , Peters LJ . What is the alpha/beta ratio for prostate cancer? rationale for hypofractionated high-dose-rate brachytherapy . Int J Radiat Oncol Biol Phys 1999. ; 44 : 747 – 8 . - PubMed
-
- Fowler J , Chappell R , Ritter M . Is alpha/beta for prostate tumors really low? Int J Radiat Oncol Biol Phys 2001. ; 50 : 1021 – 31 . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
