

Estimation of the Required Lipoprotein(a)-Lowering Therapeutic Effect Size for Reduction in Coronary Heart Disease Outcomes: A Mendelian Randomization Analysis
- PMID: 31017618
- PMCID: PMC6487909
- DOI: 10.1001/jamacardio.2019.1041
Estimation of the Required Lipoprotein(a)-Lowering Therapeutic Effect Size for Reduction in Coronary Heart Disease Outcomes: A Mendelian Randomization Analysis
Abstract
Importance: Genetic and epidemiologic data suggest that lipoprotein(a) (Lp[a]) is one of the strongest genetically determined risk factors for coronary heart disease (CHD). Specific therapies to lower Lp(a) are on the horizon, but the required reduction of Lp(a) to translate into clinically relevant lowering of CHD outcomes is a matter of debate.
Objective: To estimate the required Lp(a)-lowering effect size that may be associated with a reduction of CHD outcomes compared with the effect size of low-density lipoprotein cholesterol (LDL-C)-lowering therapies.
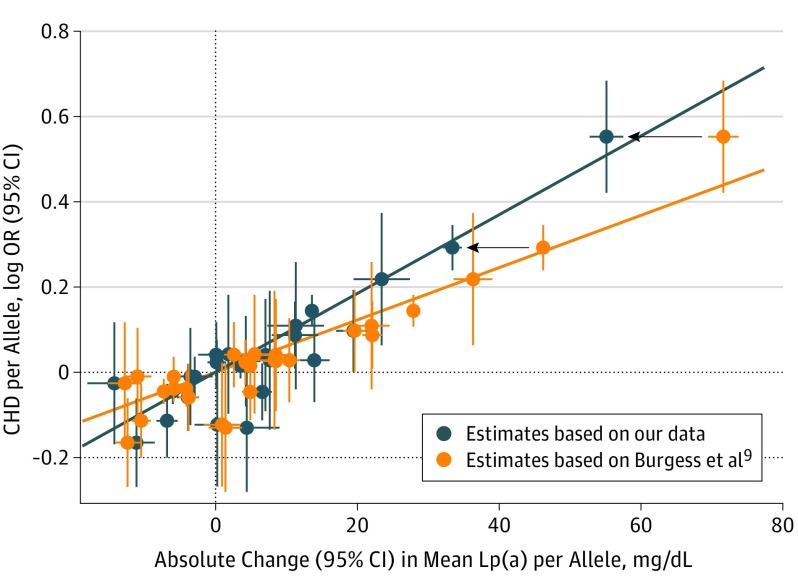
Design, setting, and participants: Genetic epidemiologic study using a mendelian randomization analysis to estimate the required Lp(a)-lowering effect size for a clinically meaningful effect on outcomes. We used the effect estimates for Lp(a) from a genome-wide association study (GWAS) and meta-analysis on Lp(a) published in 2017 of 5 different primarily population-based studies of European ancestry. All Lp(a) measurements were performed in 1 laboratory. Genetic estimates for 27 single-nucleotide polymorphisms on Lp(a) concentrations were used. Odds ratios for these 27 single-nucleotide polymorphisms associated with CHD risk were retrieved from a subsample of the CHD Exome+ consortium.
Exposures: Genetic LPA score, plasma Lp(a) concentrations, and observations of statin therapies on CHD outcomes.
Main outcomes and measures: Coronary heart disease.
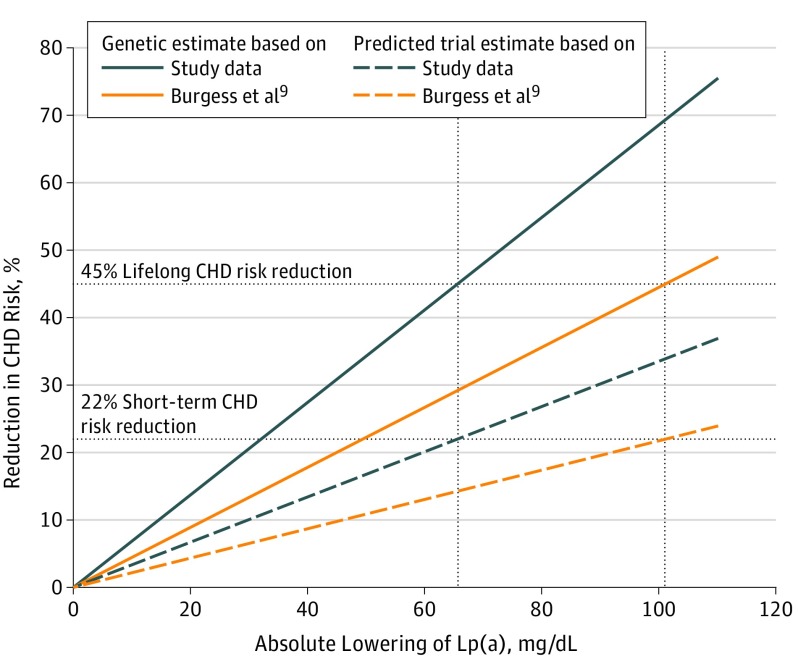
Results: The study included 13 781 individuals from the Lp(a)-GWAS-Consortium from 5 primarily population-based studies and 20 793 CHD cases and 27 540 controls from a subsample of the CHD Exome+ consortium. Four of the studies were similar in age distribution (means between 51 and 59 years), and 1 cohort was younger; mean age, 32 years. The frequency of women was similar between 51% and 55%. We estimated that the required reduction in Lp(a) effect size would be 65.7 mg/dL (95% CI, 46.3-88.3) to reach the same potential effect on clinical outcomes that can be reached by lowering LDL-C by 38.67 mg/dL (to convert to millimoles per liter, multiply by 0.0259).
Conclusions and relevance: This mendelian randomization analysis estimated a required Lp(a)-lowering effect size of 65.7 mg/dL to reach the same effect as a 38.67-mg/dL lowering of LDL-C. However, this estimate is determined by the observed effect estimates of single-nucleotide polymorphisms on Lp(a) concentrations and is therefore influenced by the standardization of the Lp(a) assay used. As a consequence, calculations of the required Lp(a)-lowering potential of a drug to be clinically effective might have been overestimated in the past.
Conflict of interest statement
Figures
Comment in
-
Using Genetics to Plan Future Randomized Trials of Lipoprotein(a) Lowering-How Much Reduction, for How Long, and in Whom?JAMA Cardiol. 2019 Jun 1;4(6):513-514. doi: 10.1001/jamacardio.2019.1107. JAMA Cardiol. 2019. PMID: 31017615 No abstract available.
-
Novel therapeutics specific to lipoprotein(a).Atherosclerosis. 2019 Sep;288:166-167. doi: 10.1016/j.atherosclerosis.2019.06.902. Epub 2019 Jun 21. Atherosclerosis. 2019. PMID: 31280874 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
