

Diaphragm sniff ultrasound: Normal values, relationship with sniff nasal pressure and accuracy for predicting respiratory involvement in patients with neuromuscular disorders
- PMID: 31017911
- PMCID: PMC6481788
- DOI: 10.1371/journal.pone.0214288
Diaphragm sniff ultrasound: Normal values, relationship with sniff nasal pressure and accuracy for predicting respiratory involvement in patients with neuromuscular disorders
Abstract
Background: In patients with neuromuscular disorders, assessment of respiratory function relies on forced vital capacity (FVC) measurements. Providing complementary respiratory outcomes may be useful for clinical trials. Diaphragm sniff ultrasound (US) is a noninvasive technique that can assess diaphragm function that may be affected in patients with neuromuscular disorders.
Purpose: We aimed to provide normal values of sniff diaphragm ultrasound, to assess the relationship between sniff diaphragm US, vital capacity (VC) and sniff nasal pressure. Additionally, we aimed to evaluate the diagnostic accuracy of sniff diaphragm US for predicting restrictive pulmonary insufficiency.
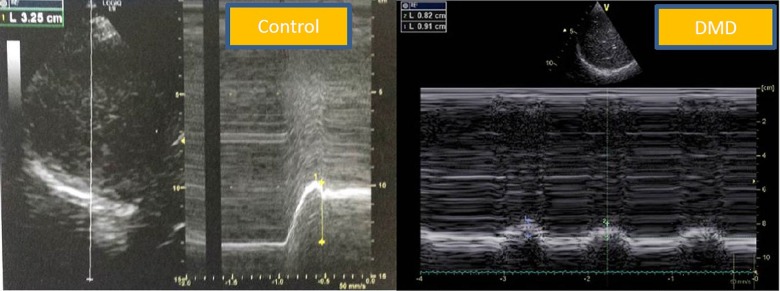
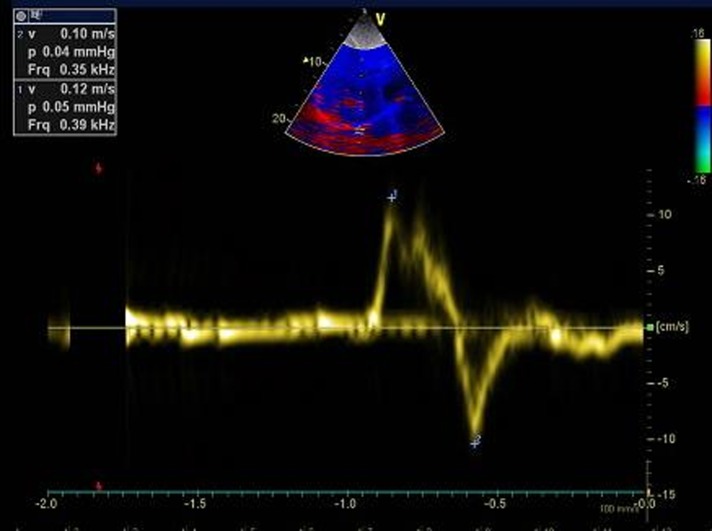
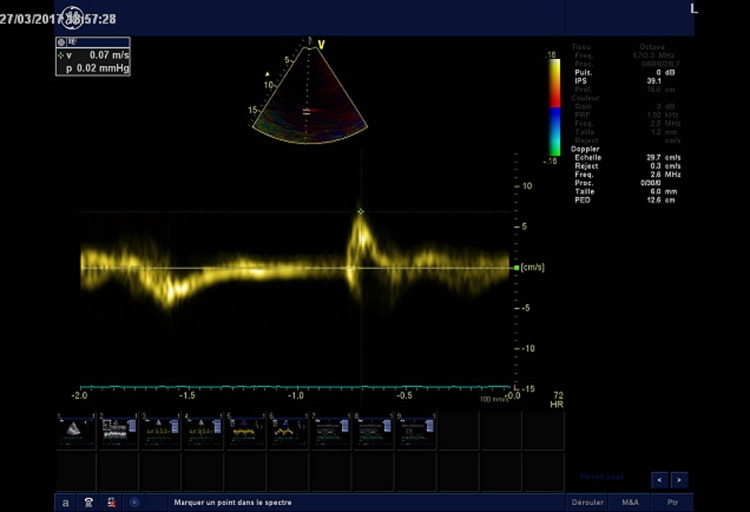
Materials and methods: We included patients with neuromuscular disorders that had been tested with a sniff diaphragm US and functional respiratory tests. Healthy subjects were also included to obtain normal diaphragm sniff ultrasound. We performed diaphragm tissue Doppler imaging (TDI) and time movement (TM) diaphragm echography combined with sniff maneuver.
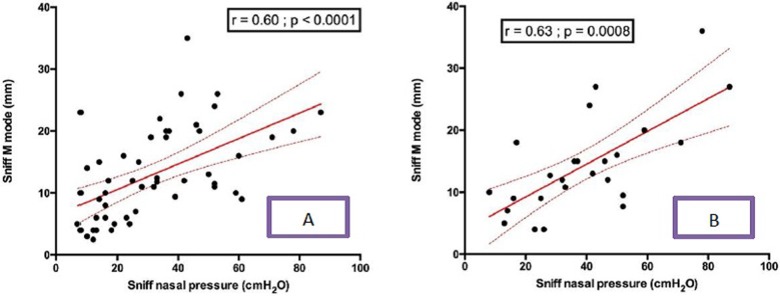
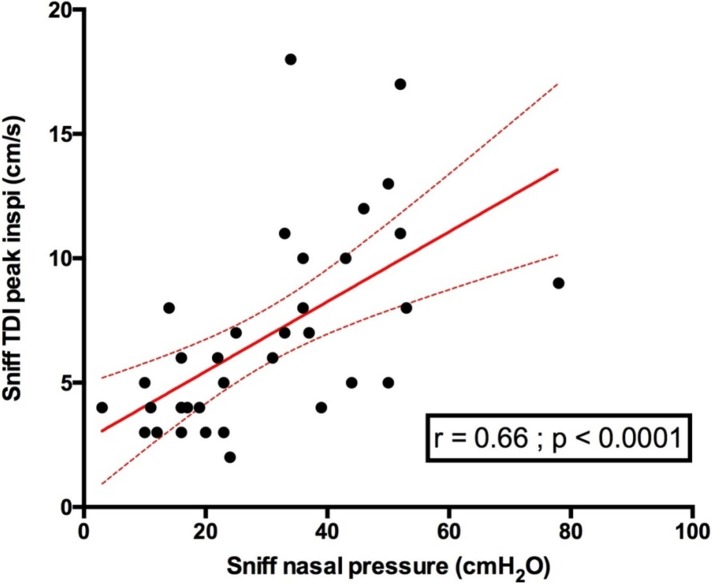
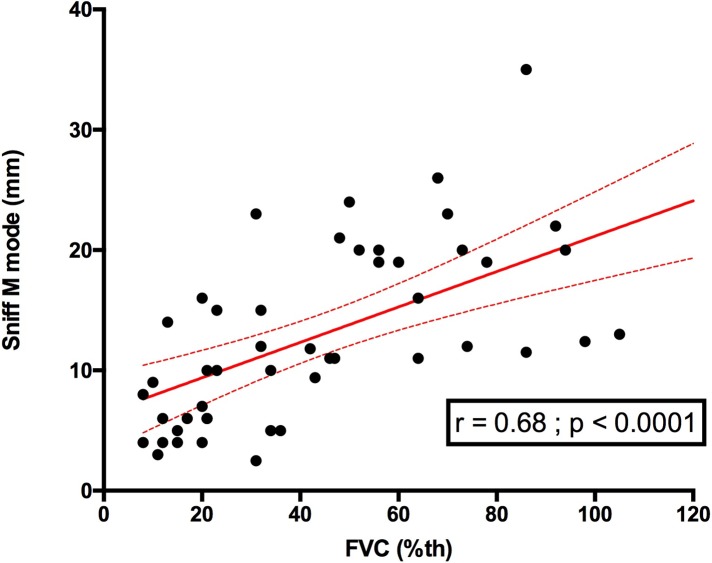
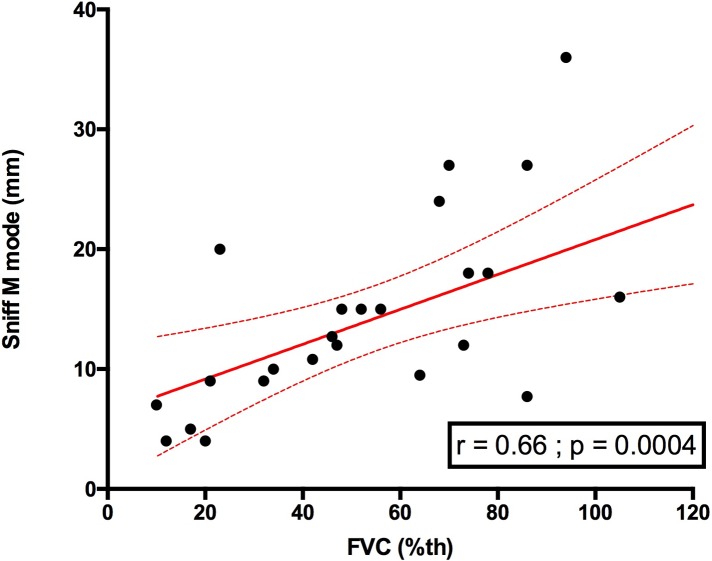
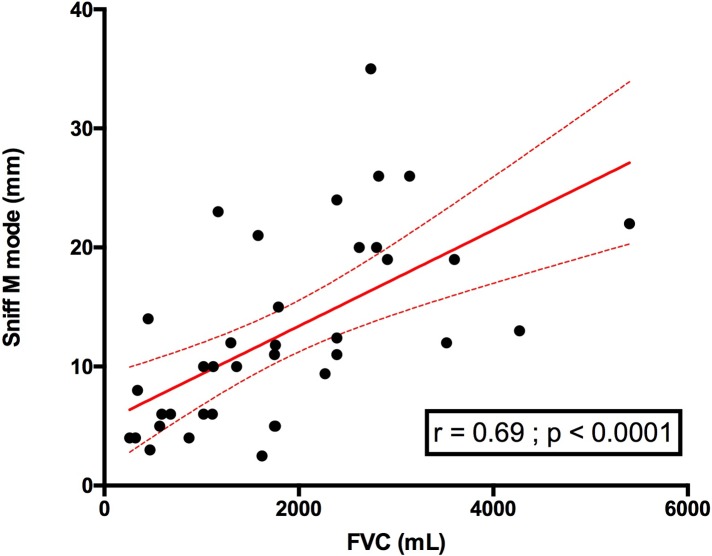
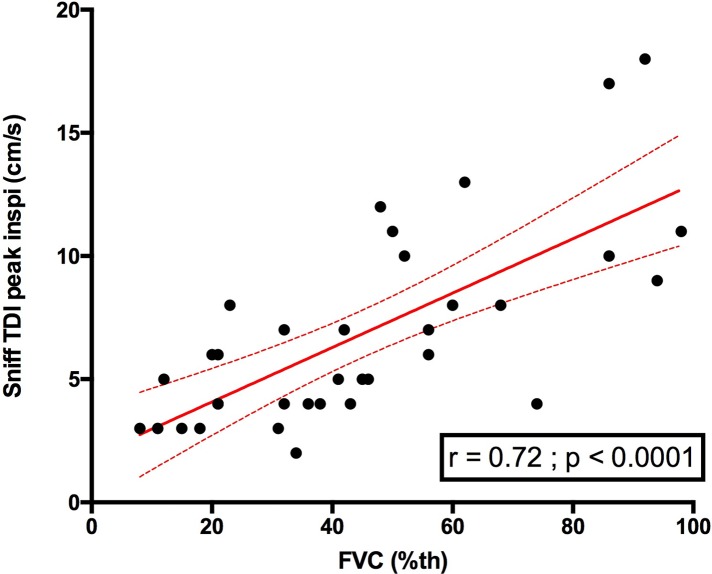
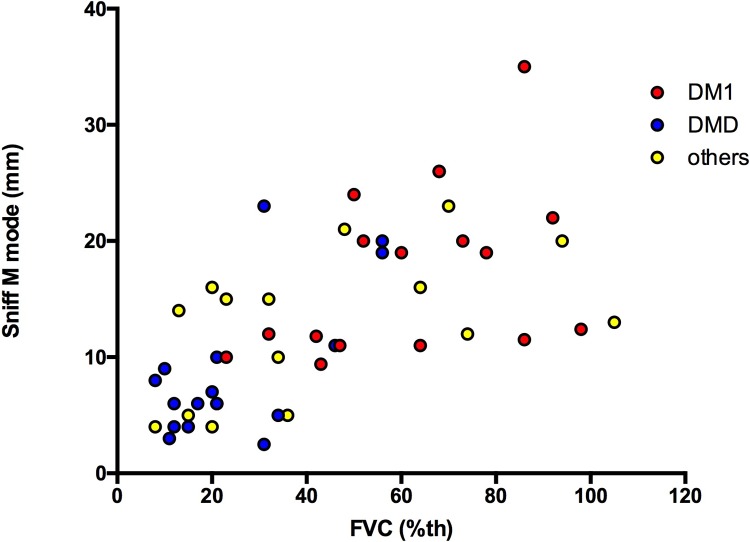
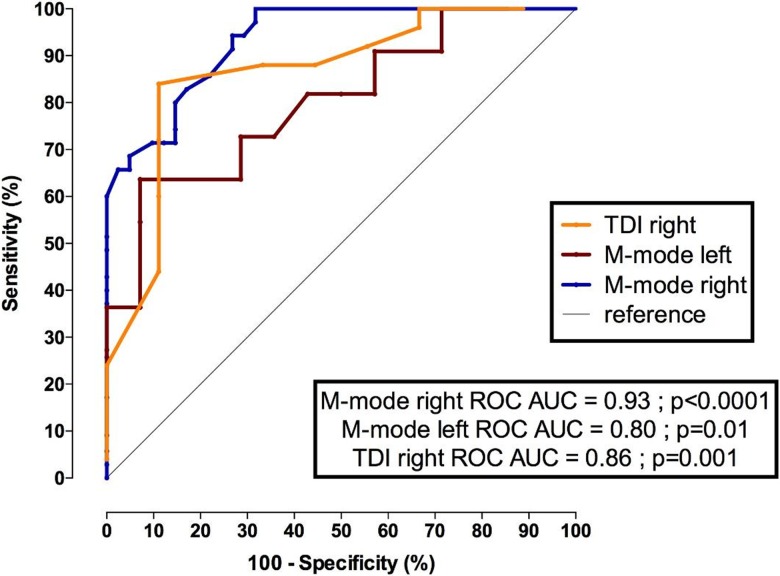
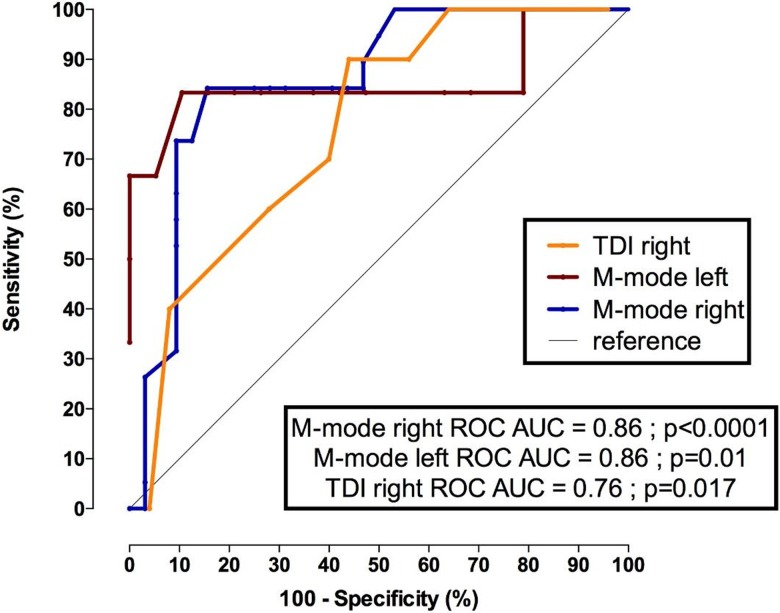
Results: A total of 89 patients with neuromuscular diseases and 27 healthy subjects were included in our study. In patients, the median age was 32 years [25; 50] and the median FVC was 34% of predicted [18; 55]. Sniff diaphragm motion using TM ultrasound was significantly associated with sniff nasal pressure, both for the right hemidiaphragm (r = 0.6 p <0.0001) and the left hemidiaphragm (r = 0.63 p = 0.0008). Right sniff peak TDI velocity was also significantly associated with FVC (r = 0.72, p<0.0001) and with sniff nasal pressure (r = 0.66 p<0.0001). Sniff diaphragm ultrasound using either TM mode or TDI displayed significant accuracy for predicting FVC<60% with an area under curve (AUC) reaching 0.93 (p<0.0001) for the right sniff diaphragm ultrasound in TM mode and 0.86 (p<0.001) for right peak diaphragm TDI velocity.
Conclusion: Sniff diaphragm TM and TDI measures were significantly associated with sniff nasal pressure. Sniff diaphragm TM and TDI had a high level of accuracy to reveal respiratory involvement in patients with neuromuscular disorders. This technique is useful to assess and follow up diaphragm function in patients with neuromuscular disorders. It may be used as a respiratory outcome for clinical trials.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Ultrasound assessment of diaphragmatic function in patients with amyotrophic lateral sclerosis.Respirology. 2016 Jul;21(5):932-8. doi: 10.1111/resp.12759. Epub 2016 Mar 19. Respirology. 2016. PMID: 26994409
-
Diaphragm: Pathophysiology and Ultrasound Imaging in Neuromuscular Disorders.J Neuromuscul Dis. 2018;5(1):1-10. doi: 10.3233/JND-170276. J Neuromuscul Dis. 2018. PMID: 29278898 Free PMC article. Review.
-
Noninvasive measurement of the maximum relaxation rate of inspiratory muscles in patients with neuromuscular disorders.Respiration. 2006;73(4):474-80. doi: 10.1159/000091804. Epub 2006 Feb 27. Respiration. 2006. PMID: 16508243
-
Sniff nasal inspiratory pressure and sleep disordered breathing in childhood neuromuscular disorders.Neuromuscul Disord. 2012 Jun;22(6):528-33. doi: 10.1016/j.nmd.2012.02.002. Epub 2012 Mar 3. Neuromuscul Disord. 2012. PMID: 22386707
-
Imaging of respiratory muscles in neuromuscular disease: A review.Neuromuscul Disord. 2018 Mar;28(3):246-256. doi: 10.1016/j.nmd.2017.11.010. Epub 2017 Nov 24. Neuromuscul Disord. 2018. PMID: 29398294 Review.
Cited by
-
Ultrasound and non-ultrasound imaging techniques in the assessment of diaphragmatic dysfunction.BMC Pulm Med. 2021 Mar 15;21(1):85. doi: 10.1186/s12890-021-01441-6. BMC Pulm Med. 2021. PMID: 33722215 Free PMC article. Review.
-
Diaphragmatic ultrasound: approach, emerging evidence, and future perspectives in non-ICU patients.Intern Emerg Med. 2025 Apr;20(3):643-654. doi: 10.1007/s11739-024-03835-w. Epub 2024 Dec 13. Intern Emerg Med. 2025. PMID: 39673007 Review.
-
Breathless Strength: Ultrasonographic Insights into Expiratory Muscle Dysfunction in Spinal Cord Injury.Medicina (Kaunas). 2025 May 15;61(5):897. doi: 10.3390/medicina61050897. Medicina (Kaunas). 2025. PMID: 40428855 Free PMC article.
-
Post-Myocardial Infarction Rehabilitation: The Absence in the Rehabilitation Process of the Diaphragm Muscle.Int J Gen Med. 2024 Jul 22;17:3201-3210. doi: 10.2147/IJGM.S470878. eCollection 2024. Int J Gen Med. 2024. PMID: 39070222 Free PMC article. Review.
-
Quantitative analysis of diaphragm motion during fluoroscopic sniff test to assist in diagnosis of hemidiaphragm paralysis.Radiol Case Rep. 2022 Mar 25;17(5):1750-1754. doi: 10.1016/j.radcr.2022.02.083. eCollection 2022 May. Radiol Case Rep. 2022. PMID: 35355529 Free PMC article.
References
-
- Héritier F, Rahm F, Pasche P, Fitting JW. Sniff nasal inspiratory pressure. A noninvasive assessment of inspiratory muscle strength. Am J Respir Crit Care Med. 1994. December;150(6 Pt 1):1678–83 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
