

Biomarkers of basal cell carcinoma resistance to methyl-aminolevulinate photodynamic therapy
- PMID: 31017970
- PMCID: PMC6481917
- DOI: 10.1371/journal.pone.0215537
Biomarkers of basal cell carcinoma resistance to methyl-aminolevulinate photodynamic therapy
Abstract
Background: Methyl-aminolevulinate photodynamic therapy (MAL-PDT) is an excellent option for the treatment of basal cell carcinoma (BCC). However, up to 25% of cases are resistant to this treatment modality.
Objective: The aim of this study was to identify potential biomarkers of BCC response to MAL-PDT.
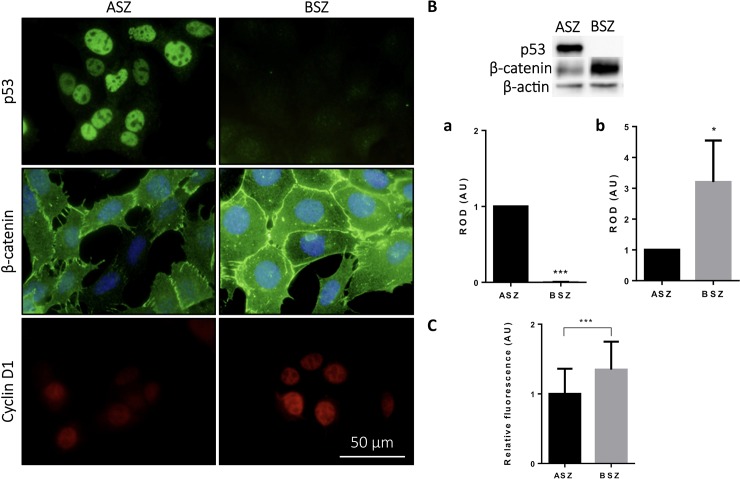
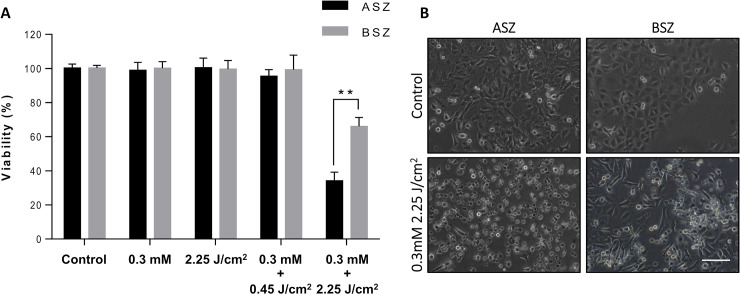
Material and methods: Clinical, histological, and immunohistochemical (p53, Ki-67, CD-31, COX2, β-catenin, EGFR, and survivin) variables were analyzed in a retrospective study of consecutive BCC patients treated with MAL-PDT at the San Jorge Hospital, Huesca, Spain between January 2006 and December 2015. To deepen on these markers, the effects on p53 and cyclin D1 expression, in vitro response to MAL-PDT of 2 murine BCC cell lines (ASZ and BSZ), was also evaluated.
Results: The retrospective study examined the response to MAL-PDT of 390 BCCs from 182 patients. The overall clinical response rate was 82.8%, with a mean follow-up time of 35.96 months (SD = 23.46). Immunohistochemistry revealed positive p53 in 84.6% of responders but only 15.4% of nonresponsive tumors (p = 0.011). Tumors with increased peripheral palisading of basal cell islands to immunostaining β-catenin responded poorly to PDT (p = 0.01). In line with our findings in patients, in vitro studies revealed a better response to PDT in the p53-positive ASZ cell line than the p53-negative BSZ cell line (p<0.01). Multivariate analysis revealed that the following variables were significantly associated with response to PDT: age, nBCC, presence of peritumoral inflammatory infiltrate, and p53 immunopositivity. Patients with positive p53 immunostaining were 68.54 times more likely to achieve cure than p53-negative patients (CI95% 2.94-159.8).
Conclusion: Our finding suggest that certain clinicopathological and immunohistochemical variables, particularly p53 expression, may serve as indicators of BCC response to MAL-PDT, and thus facilitate the selection of patients who are most likely to benefit from this therapy.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Morton C, Szeimies RM, Sidoroff A, et al. European dermatology forum guidelines on topical photodynamic therapy. Eur J Dermatology. 2015; 25: 296–311. - PubMed
-
- Gracia-Cazana T, Salazar N, Zamarrón A, Mascaraque M, Lucena S, Juarranz A. Resistance of Nonmelanoma Skin Cancer to Nonsurgical Treatments. Part II: Photodynamic Therapy, Vismodegib, Cetuximab, Intralesional Methotrexate, and Radiotherapy. Actas Dermosifiliogr 2016; 107: 740–750. 10.1016/j.ad.2016.04.020 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
