

A retrospective alternative for active surveillance trials for ductal carcinoma in situ of the breast
- PMID: 31018242
- PMCID: PMC7004157
- DOI: 10.1002/ijc.32362
A retrospective alternative for active surveillance trials for ductal carcinoma in situ of the breast
Abstract
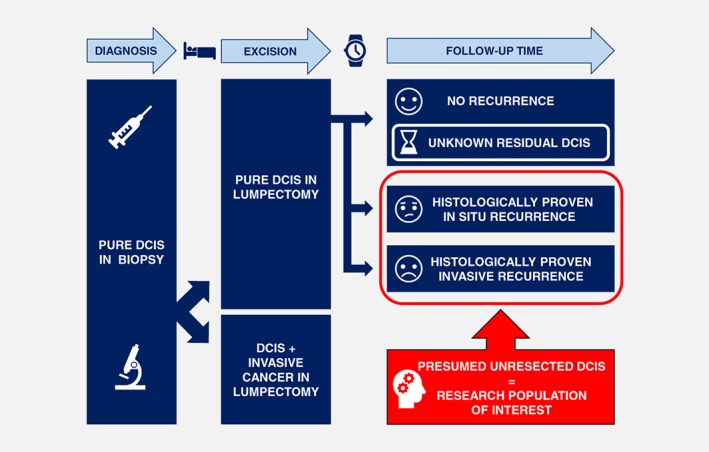
Ductal carcinoma in situ (DCIS) of the breast is a nonobligate precursor of invasive breast cancer, accounting for 20 % of screen-detected breast cancers. Little is known about the natural progression of DCIS because most patients undergo surgery upon diagnosis. Many DCIS patients are likely being overtreated, as it is believed that only around 50 % of DCIS will progress to invasive carcinoma. Robust prognostic markers for progression to invasive carcinoma are lacking. In the past, studies have investigated women who developed a recurrence after breast-conserving surgery (BCS) and compared them with those who did not. However, where there is no recurrence, the patient has probably been adequately treated. The present narrative review advocates a new research strategy, wherein only those patients with a recurrence are studied. Approximately half of the recurrences are invasive cancers, and half are DCIS. So-called "recurrences" are probably most often the result of residual disease. The new approach allows us to ask: why did some residual DCIS evolve to invasive cancers and others not? This novel strategy compares the group of patients that developed in situ recurrence with the group of patients that developed invasive recurrence after BCS. The differences between these groups could then be used to develop a robust risk stratification tool. This tool should estimate the risk of synchronous and metachronous invasive carcinoma when DCIS is diagnosed in a biopsy. Identification of DCIS patients at low risk for developing invasive carcinoma will individualize future therapy and prevent overtreatment.
Keywords: active surveillance; ductal carcinoma in situ; prognostic markers; recurrence; risk stratification.
© 2019 The Authors. International Journal of Cancer published by John Wiley & Sons Ltd on behalf of UICC.
Figures
Similar articles
-
Patterns of invasive recurrence among patients originally treated for ductal carcinoma in situ by breast-conserving surgery versus mastectomy.Breast Cancer Res Treat. 2021 Apr;186(3):617-624. doi: 10.1007/s10549-021-06129-3. Epub 2021 Mar 6. Breast Cancer Res Treat. 2021. PMID: 33675490 Free PMC article. Review.
-
Comparison of ipsilateral breast tumor recurrence after breast-conserving surgery between ductal carcinoma in situ and invasive breast cancer.World J Surg Oncol. 2016 Apr 27;14:126. doi: 10.1186/s12957-016-0885-6. World J Surg Oncol. 2016. PMID: 27122132 Free PMC article.
-
Decreasing Recurrence Rates for Ductal Carcinoma In Situ: Analysis of 2996 Women Treated with Breast-Conserving Surgery Over 30 Years.Ann Surg Oncol. 2015 Oct;22(10):3273-81. doi: 10.1245/s10434-015-4740-8. Epub 2015 Jul 28. Ann Surg Oncol. 2015. PMID: 26215193 Free PMC article.
-
Characterization and treatment of local recurrence following breast conservation for ductal carcinoma in situ.Ann Surg Oncol. 2014 Nov;21(12):3766-73. doi: 10.1245/s10434-014-3802-7. Epub 2014 May 24. Ann Surg Oncol. 2014. PMID: 24859938 Free PMC article.
-
Ductal Carcinoma In Situ - Quo Vadis?Chirurgia (Bucur). 2021 Dec;116(5 Suppl):S5-S6. Chirurgia (Bucur). 2021. PMID: 34967322 Review.
Cited by
-
Risk perception of patients with ductal carcinoma in situ (DCIS) of the breast and their healthcare practitioners: The importance of histopathological terminology, and the gaps in our knowledge.Histol Histopathol. 2025 Mar;40(3):297-306. doi: 10.14670/HH-18-806. Epub 2024 Sep 3. Histol Histopathol. 2025. PMID: 39324807 Review.
-
Grading variation in 2,934 patients with ductal carcinoma in situ of the breast: the effect of laboratory- and pathologist-specific feedback reports.Diagn Pathol. 2020 May 11;15(1):52. doi: 10.1186/s13000-020-00970-8. Diagn Pathol. 2020. PMID: 32393303 Free PMC article.
-
DCIS Progression and the Tumor Microenvironment: Molecular Insights and Prognostic Challenges.Cancers (Basel). 2025 Jun 10;17(12):1925. doi: 10.3390/cancers17121925. Cancers (Basel). 2025. PMID: 40563575 Free PMC article. Review.
-
Progression from ductal carcinoma in situ to invasive breast cancer: molecular features and clinical significance.Signal Transduct Target Ther. 2024 Apr 3;9(1):83. doi: 10.1038/s41392-024-01779-3. Signal Transduct Target Ther. 2024. PMID: 38570490 Free PMC article. Review.
-
Semaphorin-7A promotes macrophage-mediated mammary epithelial and ductal carcinoma in situ invasion.Res Sq [Preprint]. 2025 May 15:rs.3.rs-6448305. doi: 10.21203/rs.3.rs-6448305/v1. Res Sq. 2025. PMID: 40470186 Free PMC article. Preprint.
References
-
- Pang JM, Gorringe KL, Fox SB. Ductal carcinoma in situ—update on risk assessment and management. Histopathology 2016;68:96–109. - PubMed
-
- van Steenbergen LN, Voogd AC, Roukema JA, et al. Screening caused rising incidence rates of ductal carcinoma in situ of the breast. Breast Cancer Res Treat 2009;115:181–3. - PubMed
-
- Glover JA, Bannon FJ, Hughes CM, et al. Increased diagnosis and detection rates of carcinoma in situ of the breast. Breast Cancer Res Treat 2012;133:779–84. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
