

Impact of Diagnosis and Therapy on Cognitive Function in Urea Cycle Disorders
- PMID: 31018246
- PMCID: PMC6692656
- DOI: 10.1002/ana.25492
Impact of Diagnosis and Therapy on Cognitive Function in Urea Cycle Disorders
Abstract
Objective: Individuals with urea cycle disorders (UCDs) often present with intellectual and developmental disabilities. The major aim of this study was to evaluate the impact of diagnostic and therapeutic interventions on cognitive outcomes in UCDs.
Methods: This prospective, observational, multicenter study includes data from 503 individuals with UCDs who had comprehensive neurocognitive testing with a cumulative follow-up of 702 patient-years.
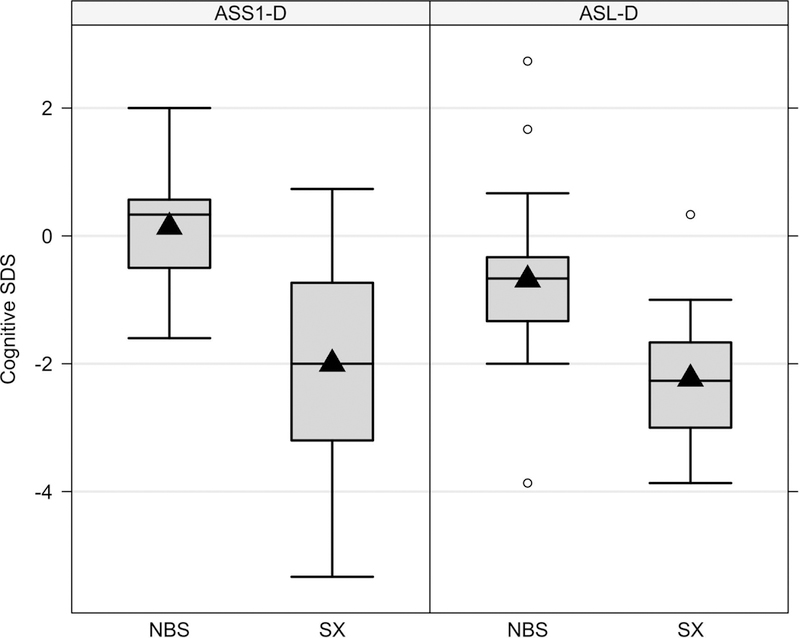
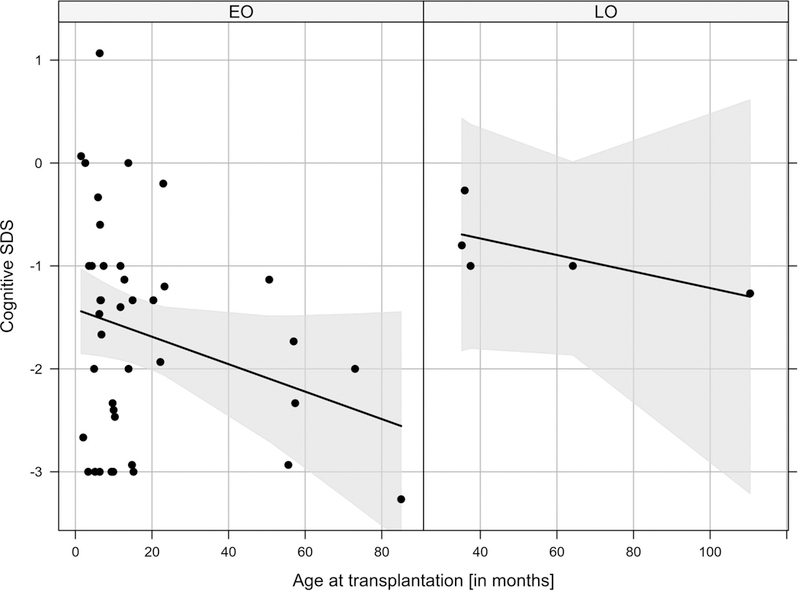
Results: The mean cognitive standard deviation score (cSDS) was lower in symptomatic than in asymptomatic (p < 0.001, t test) individuals with UCDs. Intellectual disability (intellectual quotient < 70, cSDS < -2.0) was associated with the respective subtype of UCD and early disease onset, whereas height of the initial peak plasma ammonium concentration was inversely associated with neurocognitive outcomes in mitochondrial (proximal) rather than cytosolic (distal) UCDs. In ornithine transcarbamylase and argininosuccinate synthetase 1 deficiencies, we did not find evidence that monoscavenger therapy with sodium or glycerol phenylbutyrate was superior to sodium benzoate in providing cognitive protection. Early liver transplantation appears to be beneficial for UCDs. It is noteworthy that individuals with argininosuccinate synthetase 1 and argininosuccinate lyase deficiencies identified by newborn screening had better neurocognitive outcomes than those diagnosed after the manifestation of first symptoms.
Interpretation: Cognitive function is related to interventional and non-interventional variables. Early detection by newborn screening and early liver transplantation appear to offer greater cognitive protection, but none of the currently used nitrogen scavengers was superior with regard to long-term neurocognitive outcome. Further confirmation could determine these variables as important clinical indicators of neuroprotection for individuals with UCDs. ANN NEUROL 2019.
© 2019 American Neurological Association.
Conflict of interest statement
Potential Conflicts of Interest
All other authors declare that they have nothing to report.
Figures





Similar articles
-
Suggested guidelines for the diagnosis and management of urea cycle disorders: First revision.J Inherit Metab Dis. 2019 Nov;42(6):1192-1230. doi: 10.1002/jimd.12100. Epub 2019 May 15. J Inherit Metab Dis. 2019. PMID: 30982989 Review.
-
Understanding the Natural History and the Effects of Current Therapeutic Strategies on Urea Cycle Disorders: Insights from the UCD Spanish Registry.Nutrients. 2025 Mar 28;17(7):1173. doi: 10.3390/nu17071173. Nutrients. 2025. PMID: 40218931 Free PMC article.
-
Age at disease onset and peak ammonium level rather than interventional variables predict the neurological outcome in urea cycle disorders.J Inherit Metab Dis. 2016 Sep;39(5):661-672. doi: 10.1007/s10545-016-9938-9. Epub 2016 Apr 22. J Inherit Metab Dis. 2016. PMID: 27106216
-
Neuropsychological attributes of urea cycle disorders: A systematic review of the literature.J Inherit Metab Dis. 2019 Nov;42(6):1176-1191. doi: 10.1002/jimd.12146. Epub 2019 Aug 1. J Inherit Metab Dis. 2019. PMID: 31268178 Free PMC article.
-
Clinical outcomes of neonatal onset proximal versus distal urea cycle disorders do not differ.J Pediatr. 2013 Feb;162(2):324-9.e1. doi: 10.1016/j.jpeds.2012.06.065. Epub 2012 Aug 15. J Pediatr. 2013. PMID: 22901741 Free PMC article.
Cited by
-
Urea cycle defects in adulthood: clinical presentation, diagnosis and treatment in genetically encoded hepatic metabolic disorders with a potential for encephalopathy.Metab Brain Dis. 2025 Apr 26;40(5):192. doi: 10.1007/s11011-025-01619-5. Metab Brain Dis. 2025. PMID: 40285952 Free PMC article. Review.
-
Long-term effects of medical management on growth and weight in individuals with urea cycle disorders.Sci Rep. 2020 Jul 20;10(1):11948. doi: 10.1038/s41598-020-67496-3. Sci Rep. 2020. PMID: 32686765 Free PMC article.
-
The landscape of CRISPR/Cas9 for inborn errors of metabolism.Mol Genet Metab. 2023 Jan;138(1):106968. doi: 10.1016/j.ymgme.2022.106968. Epub 2022 Dec 7. Mol Genet Metab. 2023. PMID: 36525790 Free PMC article. Review.
-
Urea cycle disorders and indications for liver transplantation.Front Pediatr. 2023 Mar 3;11:1103757. doi: 10.3389/fped.2023.1103757. eCollection 2023. Front Pediatr. 2023. PMID: 36937980 Free PMC article.
-
Glycerol phenylbutyrate efficacy and safety from an open label study in pediatric patients under 2 months of age with urea cycle disorders.Mol Genet Metab. 2021 Jan;132(1):19-26. doi: 10.1016/j.ymgme.2020.12.002. Epub 2020 Dec 23. Mol Genet Metab. 2021. PMID: 33388234 Free PMC article.
References
-
- Kido J, Nakamura K, Mitsubuchi H, et al. Long-term outcome and intervention of urea cycle disorders in Japan. J Inherit Metab Dis. 2012. September;35(5):777–85. - PubMed
-
- Burgard P, Kolker S, Haege G, Lindner M, Hoffmann GF. Neonatal mortality and outcome at the end of the first year of life in early onset urea cycle disorders--review and meta-analysis of observational studies published over more than 35 years. J Inherit Metab Dis. 2016. March;39(2):219–29. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U54HD090257/NH/NIH HHS/United States
- 2010 12 01/European Union/International
- Physician-Scientist Program at University of Heidelberg/International
- National Urea Cycle Disorders Foundation/International
- Dietmar Hopp Foundation/International
- National Center for Advancing Translational Science/International
- U54 HD061221/HD/NICHD NIH HHS/United States
- Rotenberg Family Fund/International
- radiz-Rare Disease Initiative Zurich/International
- EAHC no 2010 12 01/European Union/International
- Kettering Fund/International
- Eunice Kennedy Shriver National Institute of Child Health and Human Development/International
- U54 HD086984/HD/NICHD NIH HHS/United States
- Heidelberg Research Center for Molecular Medicine (HRCMM) in the framework of the Excellence Initiative II of the German Research Foundation/International
- Office of Rare Diseases Research/International
- U2C TR002818/TR/NCATS NIH HHS/United States
- O'Malley Foundation/International
- Kindness-for-Kids Foundation/International
- U54 HD090257/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
