

Combined Microsurgery and Endovascular Intervention in One-Stop for Treatment of Cerebral Arteriovenous Malformation: The Efficacy of a Hybrid Operation
- PMID: 31018668
- PMCID: PMC6728716
- DOI: 10.1177/0963689719845366
Combined Microsurgery and Endovascular Intervention in One-Stop for Treatment of Cerebral Arteriovenous Malformation: The Efficacy of a Hybrid Operation
Abstract
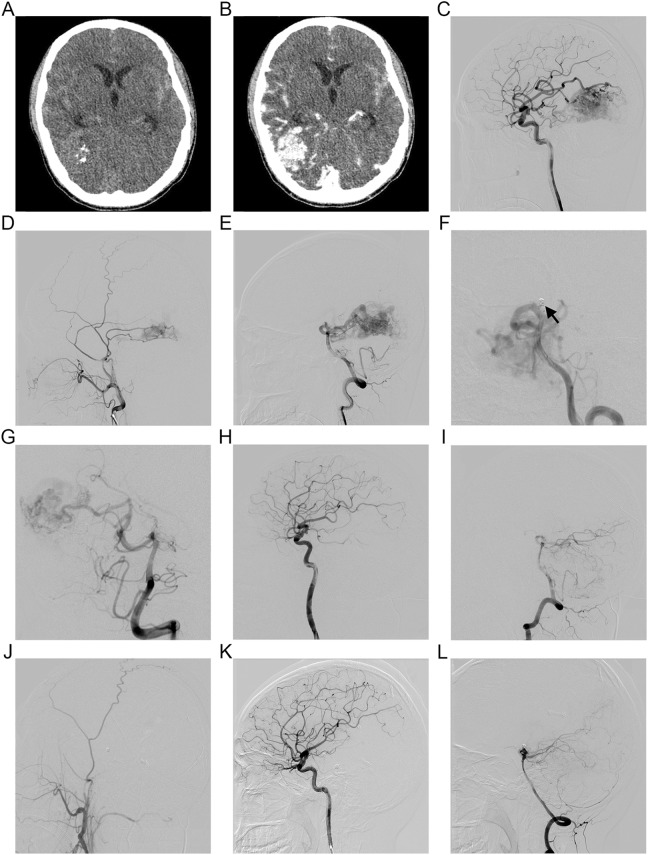
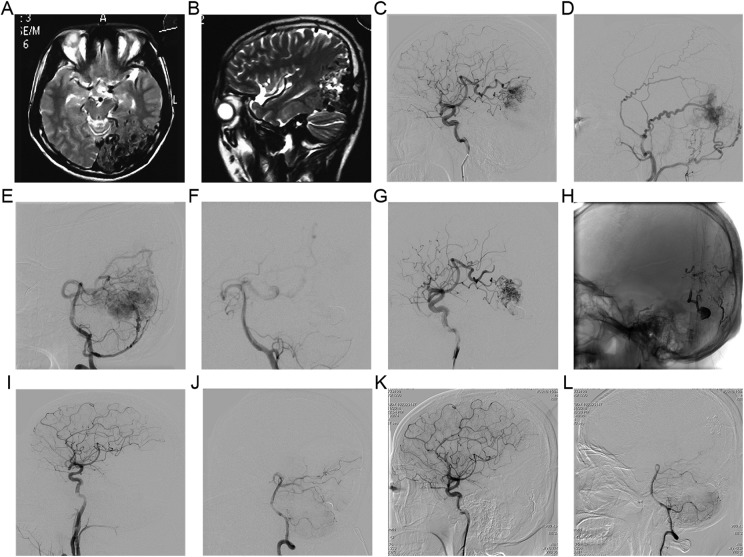
To investigate the efficacy of a hybrid operation combining microsurgical resection and endovascular interventions in a one-stop treatment of cerebral arteriovenous malformation (AVM). Patients were divided into two groups: patients who received a hybrid operation, and patients receiving a non-hybrid operation. The hybrid operation group consisted of microsurgical resection with intraoperative angiography, or endovascular embolization. The non-hybrid operation group consisted of microsurgical resection or endovascular embolization, or microsurgery combined with embolization in multiple steps. Comprehensive clinical data was collected for all patients, including preoperative Glasgow Coma Scale score, Spetzler-Martin grade, rehemorrhagia, image follow-up, and 6-month outcomes of the modified Rankin Scale (mRS) score. This study included 22 cases in the hybrid operation group. The remnants were noted on intraoperative angiography in the four patients that were resected within the same session. The non-hybrid group consisted of 52 patients. There were no statistical differences between the two groups with GCS and Spetzler-Martin grade score. The mortality rate in the hybrid operation group was 4.5%, which was lower than the 7.6% obtained in the control group. No patients experienced post-operation rehemorrhagia in the hybrid operation group, but five cases occurred in the control group. The follow-up radiological cure rates were 100% in the hybrid group and 65.9% in the control group. The rate of good outcome was 81.8% in the hybrid operation group and 69.2% in the control group, although there was no significant difference. The hybrid operation is a safe and efficacious strategy for treating cerebral AVMs.
Keywords: cerebral arteriovenous malformation; hybrid operation; one-stop.
Conflict of interest statement
Figures
Similar articles
-
Microsurgery for cerebral arteriovenous malformations: subgroup outcomes in a consecutive series of 288 cases.J Neurosurg. 2017 Apr;126(4):1056-1063. doi: 10.3171/2016.4.JNS153017. Epub 2016 Jun 10. J Neurosurg. 2017. PMID: 27285541 Clinical Trial.
-
Safety and outcome of combined endovascular and surgical management of low grade cerebral arteriovenous malformations in children compared to surgery alone.Eur J Radiol. 2019 Jul;116:8-13. doi: 10.1016/j.ejrad.2019.02.016. Epub 2019 Feb 18. Eur J Radiol. 2019. PMID: 31153578
-
Combined Endovascular and Microsurgical Treatment of Arteriovenous Malformations in the Hybrid Operating Room.World Neurosurg. 2018 Sep;117:e204-e214. doi: 10.1016/j.wneu.2018.05.241. Epub 2018 Jun 8. World Neurosurg. 2018. PMID: 29890278
-
[Differential therapy of cerebral arteriovenous malformations. An analysis with reference to personal microsurgery experiences].Nervenarzt. 1996 Oct;67(10):860-9. doi: 10.1007/s001150050063. Nervenarzt. 1996. PMID: 9036359 Review. German.
-
Transvenous embolization of brain arteriovenous malformations: a review of techniques, indications, and outcomes.Neurosurg Focus. 2018 Jul;45(1):E13. doi: 10.3171/2018.3.FOCUS18113. Neurosurg Focus. 2018. PMID: 29961383 Review.
Cited by
-
Hybrid Operative Room for Vascular Neurosurgery: Applications, Limits, and Perspectives.Adv Tech Stand Neurosurg. 2025;55:153-163. doi: 10.1007/978-3-031-90762-3_8. Adv Tech Stand Neurosurg. 2025. PMID: 40608105 Review.
-
Peri-procedure efficacy and safety of one-stop hybrid surgery for the treatment of brain arteriovenous malformations: A single-center preliminary experience.Front Neurol. 2022 Nov 4;13:1052882. doi: 10.3389/fneur.2022.1052882. eCollection 2022. Front Neurol. 2022. PMID: 36408526 Free PMC article.
-
Combined open revascularization and endovascular treatment of complex intracranial aneurysms: case series.Front Neurol. 2023 Apr 21;14:1102496. doi: 10.3389/fneur.2023.1102496. eCollection 2023. Front Neurol. 2023. PMID: 37153667 Free PMC article.
-
Enhancing the quality of evidence, comparability, and reproducibility in brain arteriovenous malformations treated with open surgery research: a systematic review and proposal of a reporting guideline for surgical and clinical outcomes.Neurosurg Rev. 2024 Apr 21;47(1):174. doi: 10.1007/s10143-024-02422-z. Neurosurg Rev. 2024. PMID: 38643293
References
-
- Ogilvy CS, Stieg PE, Awad I, Brown RJ, Kondziolka D, Rosenwasser R, Young WL, Hademenos G. Recommendations for the management of intracranial arteriovenous malformations: a statement for healthcare professionals from a special writing group of the Stroke Council, American Stroke Association. Circulation. 2001;103(21):2644–2657. - PubMed
-
- Spetzler RF, Martin NA. A proposed grading system for arteriovenous malformations. J Neurosurg. 1986;65(4):476–483. - PubMed
-
- Ellis TL, Friedman WA, Bova FJ, Kubilis PS, Buatti JM. Analysis of treatment failure after radiosurgery for arteriovenous malformations. J Neurosurg. 1998;89(1):104–110. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
