

Developing a toolkit to implement the Statin Choice Conversation Aid at scale: application of a work reduction model
- PMID: 31018840
- PMCID: PMC6480421
- DOI: 10.1186/s12913-019-4055-8
Developing a toolkit to implement the Statin Choice Conversation Aid at scale: application of a work reduction model
Abstract
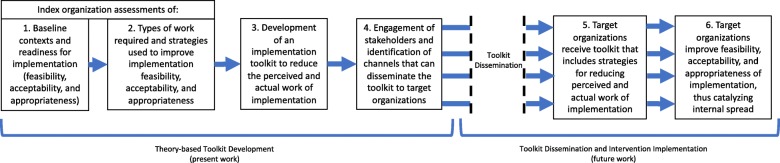
Background: Guidelines recommend shared decision making (SDM) for determining whether to use statins to prevent cardiovascular events in at-risk patients. We sought to develop a toolkit to facilitate the cross-organizational spread and scale of a SDM intervention called the Statin Choice Conversation Aid (SCCA) by (i) assessing the work stakeholders must do to implement the tool; and (ii) orienting the resulting toolkit's components to communicate and mitigate this work.
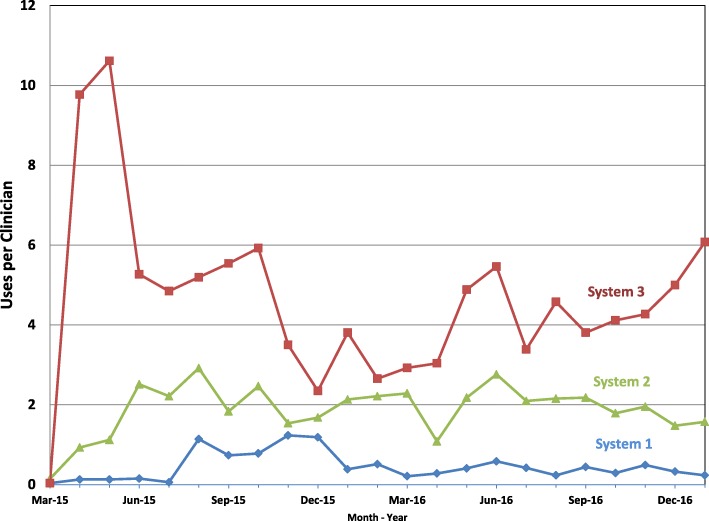
Methods: We conducted multi-level and mixed methods (survey, interview, observation, focus group) characterizations of the contexts of 3 health systems (n = 86, 84, and 26 primary care clinicians) as they pertained to the impending implementation of the SCCA. We merged the data within implementation outcome domains of feasibility, appropriateness, and acceptability. Using Normalization Process Theory, we then characterized and categorized the work stakeholders did to implement the tool. We used clinician surveys and IP address-based tracking to calculate SCCA usage over time and judged how stakeholder effort was allocated to influence outcomes at 6 and 18 months. After assessing the types and impact of the work, we developed a multi-component toolkit.
Results: At baseline, the three contexts differed regarding feasibility, acceptability, and appropriateness of implementation. The work of adopting the tool was allocated across many strategies in complex and interdependent ways to optimize these domains. The two systems that allocated the work strategically had higher uptake (5.2 and 2.9 vs. 1.1 uses per clinician per month at 6 months; 3.8 and 2.1 vs. 0.4 at 18 months, respectively) than the system that did not. The resulting toolkit included context self-assessments intended to guide stakeholders in considering the early work of SCCA implementation; and webinars, EMR integration guides, video demonstrations, and an implementation team manual aimed at supporting this work.
Conclusions: We developed a multi-component toolkit for facilitating the scale-up and spread of a tool to promote SDM across clinical settings. The theory-based approach we employed aimed to distinguish systems primed for adoption and support the work they must do to achieve implementation. Our approach may have value in orienting the development of multi-component toolkits and other strategies aimed at facilitating the efficient scale up of interventions.
Trial registration: ClinicalTrials.gov NCT02375815 .
Keywords: Implementation; Implementation strategies; Implementation toolkit; Scale-up; Shared decision making; Spread; Statin choice conversation aid; Statin choice decision aid; Statins.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Mayo Clinic Institutional Review Board and all participants gave consent to participate in this study. The reference number for the study is: 14–006048.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Beyond pros and cons - developing a patient decision aid to cultivate dialog to build relationships: insights from a qualitative study and decision aid development.BMC Med Inform Decis Mak. 2019 Sep 18;19(1):186. doi: 10.1186/s12911-019-0898-5. BMC Med Inform Decis Mak. 2019. PMID: 31533828 Free PMC article.
-
Normalization of a conversation tool to promote shared decision making about anticoagulation in patients with atrial fibrillation within a practical randomized trial of its effectiveness: a cross-sectional study.Trials. 2020 May 12;21(1):395. doi: 10.1186/s13063-020-04305-2. Trials. 2020. PMID: 32398149 Free PMC article. Clinical Trial.
-
Impact of an interprofessional shared decision-making and goal-setting decision aid for patients with diabetes on decisional conflict--study protocol for a randomized controlled trial.Trials. 2015 Jun 27;16:286. doi: 10.1186/s13063-015-0797-8. Trials. 2015. PMID: 26116444 Free PMC article. Clinical Trial.
-
Organizational- and system-level characteristics that influence implementation of shared decision-making and strategies to address them - a scoping review.Implement Sci. 2018 Mar 9;13(1):40. doi: 10.1186/s13012-018-0731-z. Implement Sci. 2018. PMID: 29523167 Free PMC article.
-
[Shared Decision Making (SDM) - Patient and Physician as a Team].Rehabilitation (Stuttg). 2017 Jun;56(3):198-213. doi: 10.1055/s-0043-106018. Epub 2017 Jun 9. Rehabilitation (Stuttg). 2017. PMID: 28599339 Review. German.
Cited by
-
Healthcare systems collaborating to implement a shared decision-making tool in the electronic health record and build evidence on its adoption and use.Learn Health Syst. 2024 Apr 15;8(Suppl 1):e10418. doi: 10.1002/lrh2.10418. eCollection 2024 Jun. Learn Health Syst. 2024. PMID: 38883873 Free PMC article.
-
Increasing risk-concordant cardiovascular care in diverse health systems: a mixed methods pragmatic stepped wedge cluster randomized implementation trial of shared decision making (SDM4IP).Implement Sci Commun. 2021 Apr 21;2(1):43. doi: 10.1186/s43058-021-00145-6. Implement Sci Commun. 2021. PMID: 33883035 Free PMC article.
-
Crohn's disease shared decision making intervention leads to more patients choosing combination therapy: a cluster randomised controlled trial.Aliment Pharmacol Ther. 2023 Jan;57(2):205-214. doi: 10.1111/apt.17286. Epub 2022 Nov 14. Aliment Pharmacol Ther. 2023. PMID: 36377259 Free PMC article. Clinical Trial.
-
Association between Exposure to Statin Choice and Adherence to Statins: An Observational Cohort Study.Med Decis Making. 2025 Jun 24:272989X251346508. doi: 10.1177/0272989X251346508. Online ahead of print. Med Decis Making. 2025. PMID: 40553465 Free PMC article.
-
The design and development of an encounter tool to support shared decision making about preventing cardiovascular events.Prev Med Rep. 2022 Sep 19;30:101994. doi: 10.1016/j.pmedr.2022.101994. eCollection 2022 Dec. Prev Med Rep. 2022. PMID: 36203943 Free PMC article.
References
-
- Goff DC, Jr, Lloyd-Jones DM, Bennett G, Coady S, D'Agostino RB, Gibbons R, Greenland P, Lackland DT, Levy D, O'Donnell CJ, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. Circulation. 2014;129(25 Suppl 2):S49–S73. doi: 10.1161/01.cir.0000437741.48606.98. - DOI - PubMed
-
- Stone Neil J., Robinson Jennifer G., Lichtenstein Alice H., Bairey Merz C. Noel, Blum Conrad B., Eckel Robert H., Goldberg Anne C., Gordon David, Levy Daniel, Lloyd-Jones Donald M., McBride Patrick, Schwartz J. Sanford, Shero Susan T., Smith Sidney C., Watson Karol, Wilson Peter W. F. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1–S45. doi: 10.1161/01.cir.0000437738.63853.7a. - DOI - PubMed
-
- Weymiller AJ, Montori VM, Jones LA, Gafni A, Guyatt GH, Bryant SC, Christianson TJ, Mullan RJ, Smith SA. Helping patients with type 2 diabetes mellitus make treatment decisions: statin choice randomized trial. Arch Intern Med. 2007;167(10):1076–1082. doi: 10.1001/archinte.167.10.1076. - DOI - PubMed
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
