

Operational characteristics of antiretroviral therapy clinics in Zambia: a time and motion analysis
- PMID: 31018846
- PMCID: PMC6480736
- DOI: 10.1186/s12913-019-4096-z
Operational characteristics of antiretroviral therapy clinics in Zambia: a time and motion analysis
Abstract
Background: The mass scale-up of antiretroviral therapy (ART) in Zambia has taken place in the context of limited infrastructure and human resources resulting in many operational side-effects. In this study, we aimed to empirically measure current workload of ART clinic staff and patient wait times and service utilization.
Methods: We conducted time and motion (TAM) studies from both the healthcare worker (HCW) and patient perspectives at 10 ART clinics throughout Zambia. Trained personnel recorded times for consecutive discrete activities based on direct observation of clinical and non-clinical activities performed by counselors, clinical officers, nurses, and pharmacy technicians. For patient TAM, we recruited consenting patients and recorded times of arrival and departure and major ART services utilized. Data from 10 clinics were pooled to evaluate median time per patient spent for each activity and patient duration of stay in the clinic.
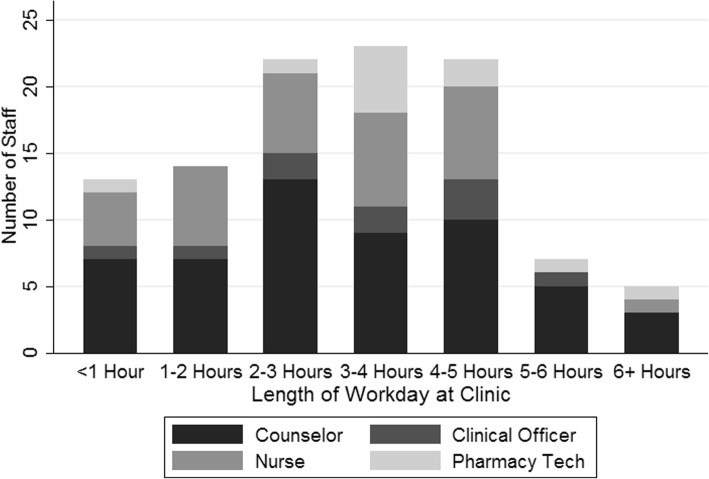
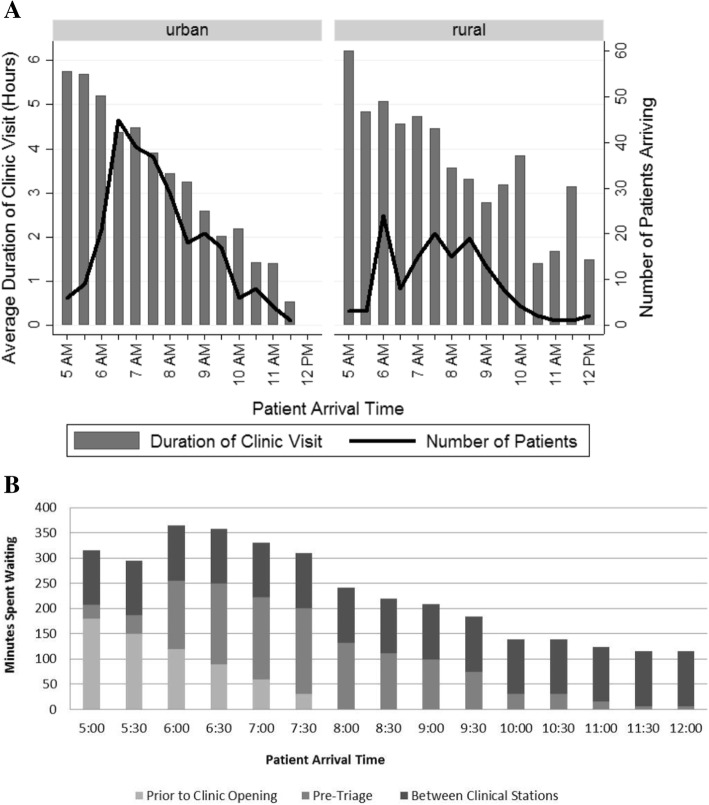
Results: The percentage of observed clinical time for direct patient interaction (median time per patient encounter) was 43.1% for ART counselors (4 min, interquartile range [IQR] 2-7), 46.1% for nurses (3 min, IQR 2-4), 57.2% for pharmacy technicians (2 min, IQR 1-2), and 78.5% for clinical officers (3 min, IQR 2-5). Patient workloads for HCWs were heaviest between 8 AM and 12 PM with few clinical activities observed after 2 PM. The length of patient visits was inversely associated with arrival time - patients arriving prior to 8 AM spent 61% longer at the clinic than those arriving after 8 AM (277 vs. 171 min). Overall, patients spent 219 min on average for non-clinical visits, and 244 min for clinical visits, but this difference was not significant in rural clinics. In comparison, total time patients spent directly with clinic staff were 9 and 12 min on average for non-clinical and clinical visits.
Conclusion: Current Zambian ART clinic operations include substantial inefficiencies for both patients and HCWs, with workloads heavily concentrated in the first few hours of clinic opening, limiting HCW and patient interaction time. Use of a differentiated care model may help to redistribute workloads during operational hours and prevent backlogs of patients waiting for hours before clinic opening, which may substantially improve ART delivery in the Zambian context.
Keywords: Allocation of resources; Antiretroviral therapy care evaluation; Antiretroviral therapy program monitoring; Program efficiency; Time and motion studies; Workload.
Conflict of interest statement
Ethics approval and consent to participate
All participants provided verbal consent, as no identifiers were collected, and provision of written consent would have increased risks to participants while also biasing the study sample. The economic evaluation study protocol, inclusive of the TAM study and verbal consent, was reviewed and approved by the Institutional Review Board in Lusaka, the University of Zambia Biomedical Research Ethics Committee (UNZA BREC).
Consent for publication
Individual data was not used in any form for this study, thus consent for publication is not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Shifting human resources for health in the context of ART provision: qualitative and quantitative findings from the Lablite baseline study.BMC Health Serv Res. 2016 Nov 16;16(1):660. doi: 10.1186/s12913-016-1891-7. BMC Health Serv Res. 2016. PMID: 27852291 Free PMC article.
-
Identifying models of HIV care and treatment service delivery in Tanzania, Uganda, and Zambia using cluster analysis and Delphi survey.BMC Health Serv Res. 2017 Dec 6;17(1):811. doi: 10.1186/s12913-017-2772-4. BMC Health Serv Res. 2017. PMID: 29207973 Free PMC article.
-
Task sharing in Zambia: HIV service scale-up compounds the human resource crisis.BMC Health Serv Res. 2010 Sep 17;10:272. doi: 10.1186/1472-6963-10-272. BMC Health Serv Res. 2010. PMID: 20849626 Free PMC article.
-
Secular trends in pediatric antiretroviral treatment programs in rural and urban Zambia: a retrospective cohort study.BMC Pediatr. 2010 Jul 30;10:54. doi: 10.1186/1471-2431-10-54. BMC Pediatr. 2010. PMID: 20673355 Free PMC article.
-
Nonadherence to antiretroviral therapy among HIV-infected patients in Zambia is concentrated among a minority of patients and is highly variable across clinics.AIDS. 2017 Mar 13;31(5):689-696. doi: 10.1097/QAD.0000000000001347. AIDS. 2017. PMID: 28225707
Cited by
-
Costs along the TB diagnostic pathway in Uganda.Int J Tuberc Lung Dis. 2021 Jan 1;25(1):61-63. doi: 10.5588/ijtld.20.0532. Int J Tuberc Lung Dis. 2021. PMID: 33384046 Free PMC article. No abstract available.
-
Human resource implications of expanding latent tuberculosis patient care activities.Front Med (Lausanne). 2024 Jan 12;10:1265476. doi: 10.3389/fmed.2023.1265476. eCollection 2023. Front Med (Lausanne). 2024. PMID: 38283039 Free PMC article.
-
A controlled study to assess the effects of a Fast Track (FT) service delivery model among stable HIV patients in Lusaka Zambia.PLOS Glob Public Health. 2022 Aug 3;2(8):e0000108. doi: 10.1371/journal.pgph.0000108. eCollection 2022. PLOS Glob Public Health. 2022. PMID: 36962510 Free PMC article.
-
Redefining and revisiting cost estimates of routine ART care in Zambia: an analysis of ten clinics.J Int AIDS Soc. 2020 Feb;23(2):e25431. doi: 10.1002/jia2.25431. J Int AIDS Soc. 2020. PMID: 32064766 Free PMC article.
-
Multicomponent strategy with decentralised molecular testing for tuberculosis in Uganda: a cost and cost-effectiveness analysis.Lancet Glob Health. 2023 Feb;11(2):e278-e286. doi: 10.1016/S2214-109X(22)00509-5. Lancet Glob Health. 2023. PMID: 36669808 Free PMC article.
References
-
- Pustil R. Global AIDS. 2016. - PubMed
-
- Ministry of Health (MOH) [Zambia] National HIV/AIDS council [Zambia]. Zambia country report: monitoring the declaration of commitment on HIV and AIDS and the universal access (global AIDS response program report) 2015.
-
- Kwena ZA, Njoroge B, Oyaro P, Cohen CR, Bukusi EA. The Feasibility and Economic Impact of Time Designated Appointment System in a Busy HIV Care Clinic. 2014;22 (Kwena, Oyaro) Center for Microbiology Research, Kenya Medical Research Institute, Kisumu, Kenya:559.
-
- Were MC, Kessler J, Shen C, Sidle J, Macharia S, Lizcano J, et al. Implementation and operational research: a time-motion analysis of HIV transmission prevention counseling and antiretroviral adherence messages in Western Kenya. J Acquir Immune Defic Syndr. 2015;69:e135–e141. doi: 10.1097/QAI.0000000000000666. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
