

Cardiac resynchronization therapy improves heart failure in one patient with acromegaly-induced cardiomyopathy: a case report
- PMID: 31018862
- PMCID: PMC6482561
- DOI: 10.1186/s13256-019-2030-y
Cardiac resynchronization therapy improves heart failure in one patient with acromegaly-induced cardiomyopathy: a case report
Abstract
Background: Congestive heart failure is rarely observed in patients with acromegaly. Excessive growth hormone secretion and elevation of insulin-like growth factor 1 contribute to pathological changes in myocyte growth and structure, cardiac contractility, vascular function, and in later stage may progress to cardiac dysfunction. Early recognition of the condition is paramount, though the insidious progression of the disease commonly results in late diagnosis. Current standard regimens of pharmacological therapy, surgical treatment, radiotherapy are designed to normalize serum levels of both insulin-like growth factor 1 and growth hormone. In patients with late-stage heart failure due to acromegalic cardiomyopathy, cardiac resynchronization therapy might be a desirable treatment to help cardiac synchronization, improve symptoms, and eventually reduce hospital admissions together with mortality rates.
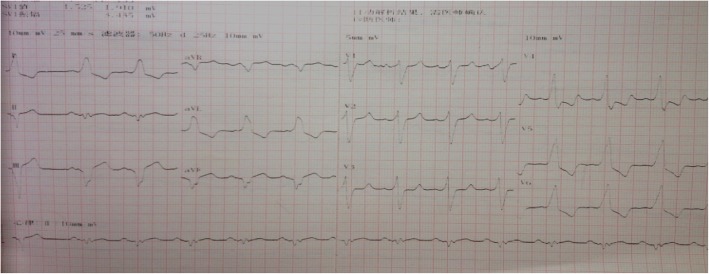
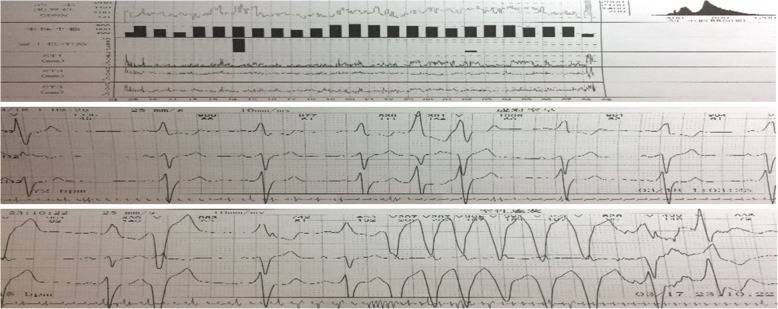
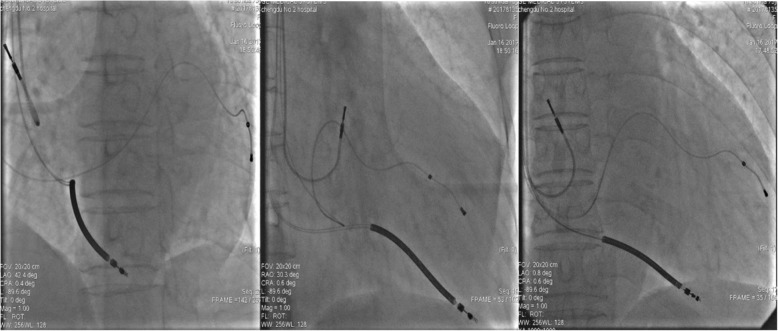
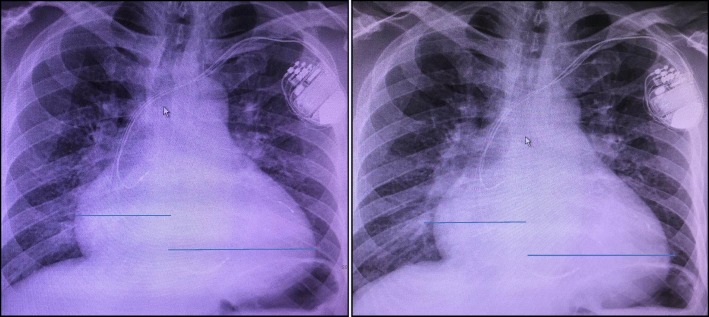
Case presentation: We describe a case of a 49-year-old man with a history of acromegaly who presented to our hospital with a diagnosis of decompensated systolic heart failure. Serial electrocardiograms showed wide (160-200 ms) QRS duration with left bundle branch block. Echocardiography showed severe left ventricular dysfunction that simultaneously achieved a left ventricular ejection fraction of 16%. Surgical indication was rarely assessed by neurosurgeons. Given that the stereotactic radiosurgery together with pharmacotherapy produced infinitesimal effects, cardiac resynchronization therapy was performed. Owing to biventricular synchronization and holding back reverse remodeling, the patient's symptoms were successfully alleviated, and he was discharged from the hospital.
Conclusions: Congestive heart failure is a rare complication in acromegaly-induced cardiomyopathy (occurs in only 3% of patients). Early diagnosis and treatment with curative drugs more than cardiovascular implantable electronic devices might lead to better surgical outcomes in this group of patients.
Keywords: Acromegalic cardiomyopathy; Cardiac resynchronization therapy; Heart failure.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
