

Chemotherapy-induced oral mucositis is associated with detrimental bacterial dysbiosis
- PMID: 31018870
- PMCID: PMC6482518
- DOI: 10.1186/s40168-019-0679-5
Chemotherapy-induced oral mucositis is associated with detrimental bacterial dysbiosis
Abstract
Background: Gastrointestinal mucosal injury (mucositis), commonly affecting the oral cavity, is a clinically significant yet incompletely understood complication of cancer chemotherapy. Although antineoplastic cytotoxicity constitutes the primary injury trigger, the interaction of oral microbial commensals with mucosal tissues could modify the response. It is not clear, however, whether chemotherapy and its associated treatments affect oral microbial communities disrupting the homeostatic balance between resident microorganisms and the adjacent mucosa and if such alterations are associated with mucositis. To gain knowledge on the pathophysiology of oral mucositis, 49 subjects receiving 5-fluorouracil (5-FU) or doxorubicin-based chemotherapy were evaluated longitudinally during one cycle, assessing clinical outcomes, bacterial and fungal oral microbiome changes, and epithelial transcriptome responses. As a control for microbiome stability, 30 non-cancer subjects were longitudinally assessed. Through complementary in vitro assays, we also evaluated the antibacterial potential of 5-FU on oral microorganisms and the interaction of commensals with oral epithelial tissues.
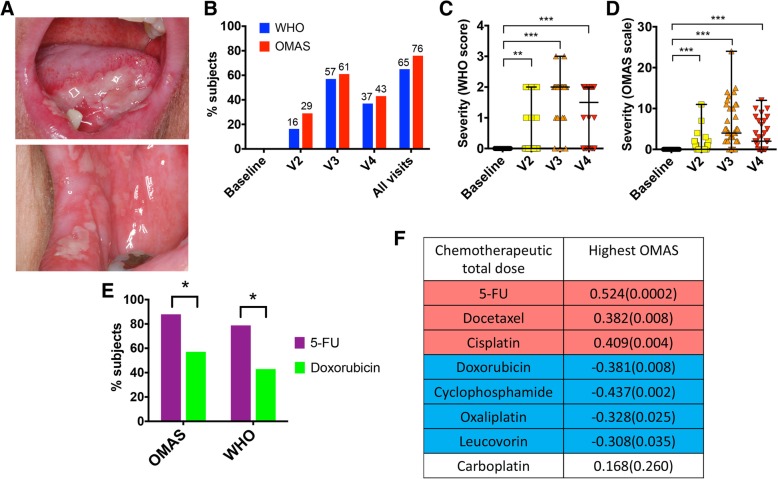
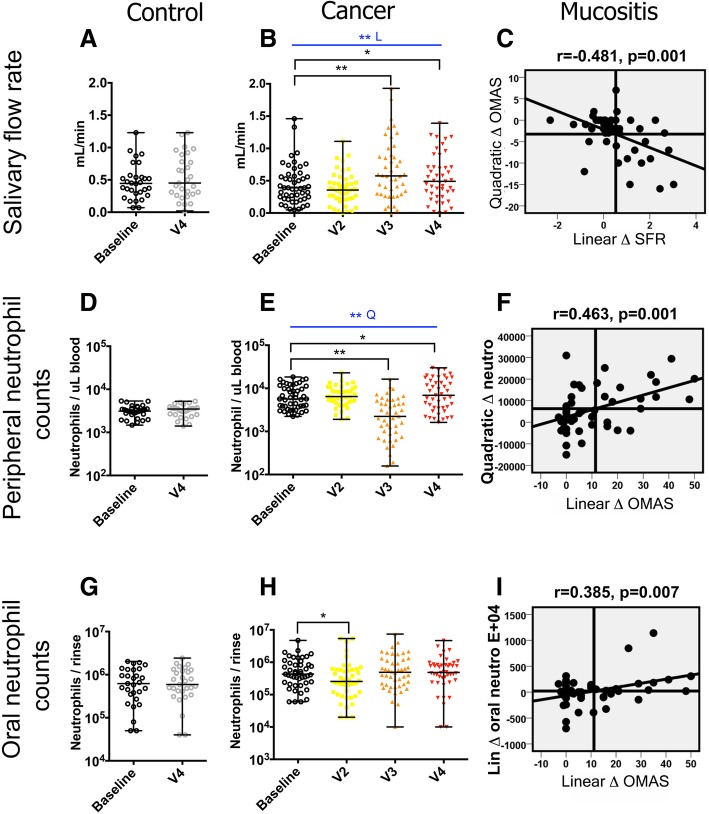
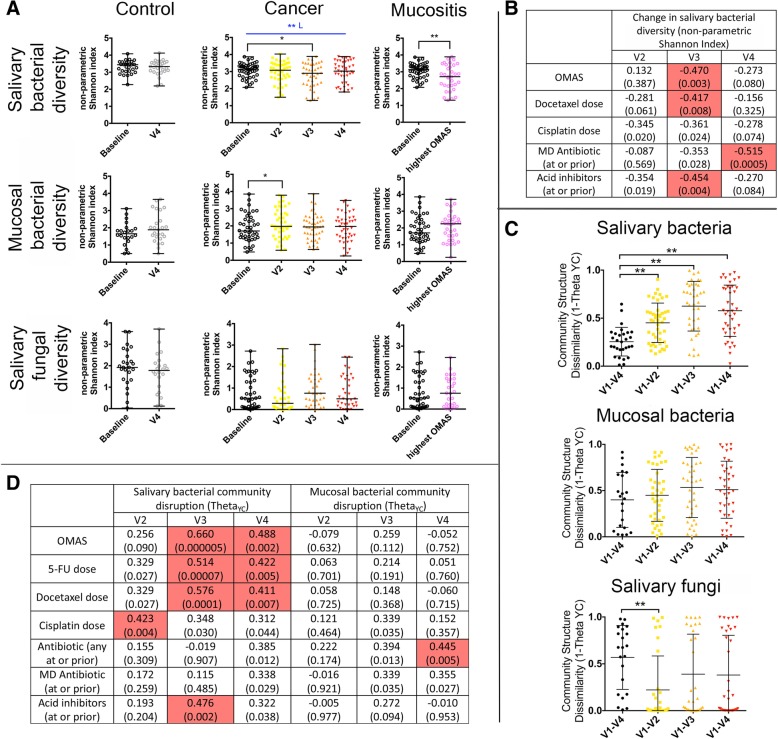
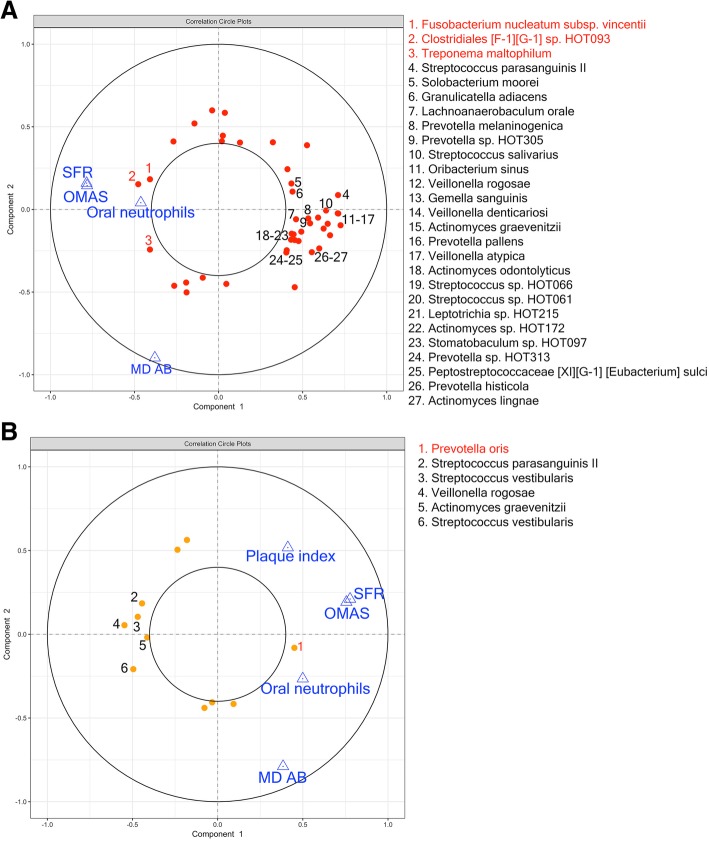
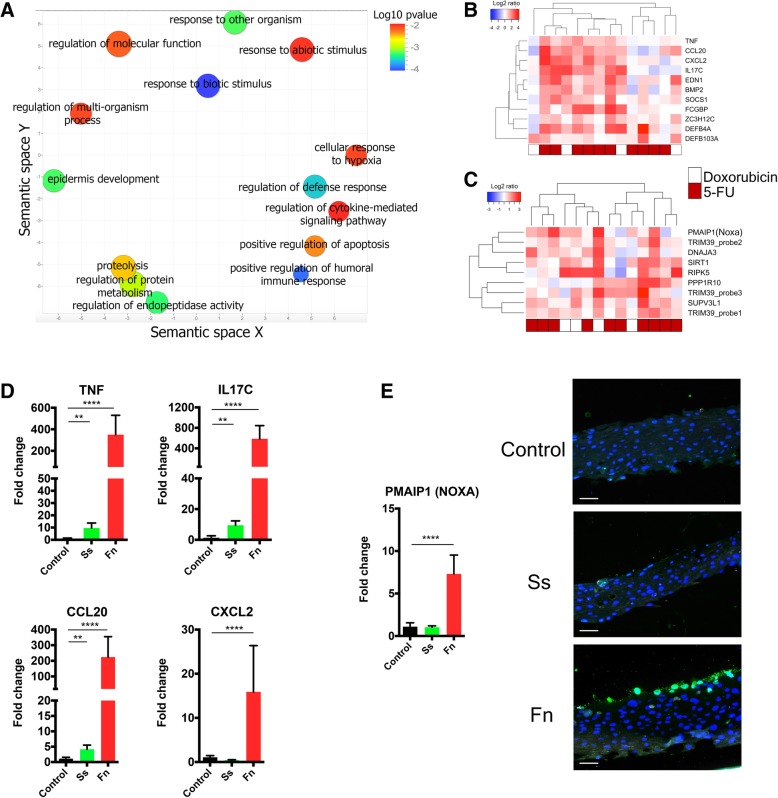
Results: Oral mucositis severity was associated with 5-FU, increased salivary flow, and higher oral granulocyte counts. The oral bacteriome was disrupted during chemotherapy and while antibiotic and acid inhibitor intake contributed to these changes, bacteriome disruptions were also correlated with antineoplastics and independently and strongly associated with oral mucositis severity. Mucositis-associated bacteriome shifts included depletion of common health-associated commensals from the genera Streptococcus, Actinomyces, Gemella, Granulicatella, and Veillonella and enrichment of Gram-negative bacteria such as Fusobacterium nucleatum and Prevotella oris. Shifts could not be explained by a direct antibacterial effect of 5-FU, but rather resembled the inflammation-associated dysbiotic shifts seen in other oral conditions. Epithelial transcriptional responses during chemotherapy included upregulation of genes involved in innate immunity and apoptosis. Using a multilayer epithelial construct, we show mucositis-associated dysbiotic shifts may contribute to aggravate mucosal damage since the mucositis-depleted Streptococcus salivarius was tolerated as a commensal, while the mucositis-enriched F. nucleatum displayed pro-inflammatory and pro-apoptotic capacity.
Conclusions: Altogether, our work reveals that chemotherapy-induced oral mucositis is associated with bacterial dysbiosis and demonstrates the potential for dysbiotic shifts to aggravate antineoplastic-induced epithelial injury. These findings suggest that control of oral bacterial dysbiosis could represent a novel preventive approach to ameliorate oral mucositis.
Keywords: Cancer; Chemotherapy; Microbiome; Mucosal-microbial crosstalk; Oral mucositis.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Institutional Review Board at UConn Health (IRB number IE-11-037 J-2). Written informed consent was received from all participants.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Murphy BA, Beaumont JL, Isitt J, Garden AS, Gwede CK, Trotti AM, et al. Mucositis-related morbidity and resource utilization in head and neck cancer patients receiving radiation therapy with or without chemotherapy. J Pain Symptom Manage. 2009;38(4):522–532. doi: 10.1016/j.jpainsymman.2008.12.004. - DOI - PubMed
-
- Rosenthal DI. Consequences of mucositis-induced treatment breaks and dose reductions on head and neck cancer treatment outcomes. J Support Oncol. 2007;5(9 Suppl 4):23–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
