

Leptomeningeal metastases in glioma: The Memorial Sloan Kettering Cancer Center experience
- PMID: 31019097
- PMCID: PMC6541431
- DOI: 10.1212/WNL.0000000000007529
Leptomeningeal metastases in glioma: The Memorial Sloan Kettering Cancer Center experience
Abstract
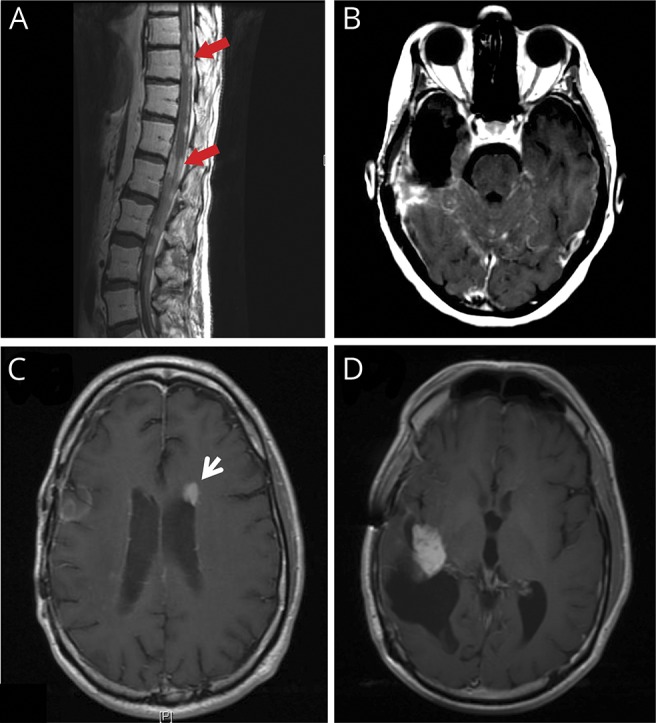
Objective: To perform a retrospective analysis examining the incidence and prognosis of glioma patients with leptomeningeal disease (LMD) at Memorial Sloan Kettering Cancer Center over a 15-year period and correlate these findings with clinicopathologic characteristics.
Methods: We conducted a retrospective review of glioma patients with LMD at Memorial Sloan Kettering Cancer Center diagnosed from 2001 to 2016. Patients were identified through a keyword search of their electronic medical record and by ICD-9 codes.
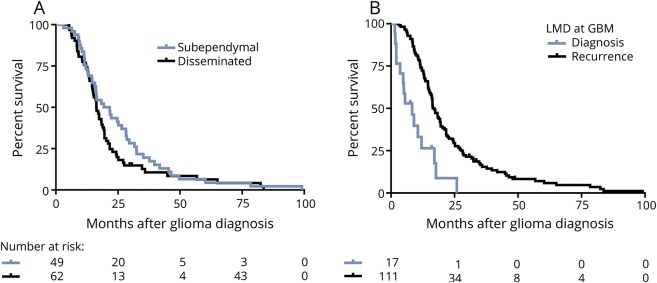
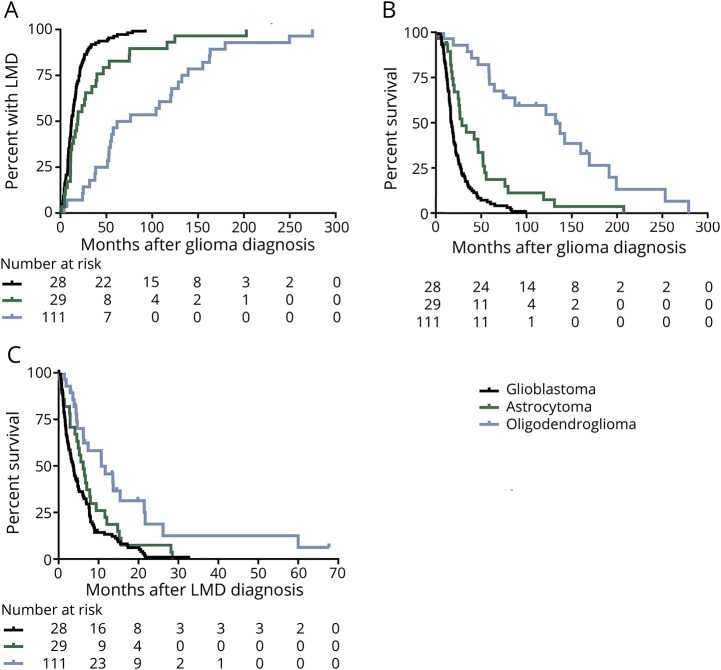
Results: One hundred three patients were identified with disseminated LMD and 85 patients with subependymal spread of disease, 4.7% of all patients with glioma. These cohorts were analyzed separately for time to development of disseminated LMD/subependymal LMD, median overall survival, and survival from LMD diagnosis. Patients were pooled for subsequent analyses (n = 188) because of comparable clinical behavior. LMD was present at glioma diagnosis in 10% of patients. In the remaining 90% of patients diagnosed at recurrence, time to LMD diagnosis, survival after LMD diagnosis, and overall survival varied by original histology. Patients with oligodendroglioma had a median survival of 10.8 (range 1.8-67.7) months, astrocytoma 6.5 (0.1-28.5) months, and glioblastoma 3.8 (0.1-32.6) months after LMD diagnosis. In addition, we found that treatment of LMD was associated with superior performance status and increased survival.
Conclusion: Patients with LMD diagnosed at relapse may not have decreased overall survival as compared to historical controls with parenchymal relapse and may benefit from treatment.
© 2019 American Academy of Neurology.
Figures
References
-
- Roldan G, Scott J, George D, et al. Leptomeningeal disease from oligodendroglioma: clinical and molecular analysis. Can J Neurol Sci 2008;35:204–209. - PubMed
-
- Lawton CD, Nagasawa DT, Yang I, Fessler RG, Smith ZA. Leptomeningeal spinal metastases from glioblastoma multiforme: treatment and management of an uncommon manifestation of disease. J Neurosurg Spine 2012;17:438–448. - PubMed
-
- Mandel JJ, Yust-Katz S, Cachia D, et al. Leptomeningeal dissemination in glioblastoma: an inspection of risk factors, treatment, and outcomes at a single institution. J Neurooncol 2014;120:597–605. - PubMed
-
- Chamberlain MC. Combined-modality treatment of leptomeningeal gliomatosis. Neurosurgery 2003;52:324–329; discussion 330. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical