

A systematic approach in the diagnosis of paediatric skull lesions: what radiologists need to know
- PMID: 31019602
- PMCID: PMC6479152
- DOI: 10.5114/pjr.2019.83101
A systematic approach in the diagnosis of paediatric skull lesions: what radiologists need to know
Abstract
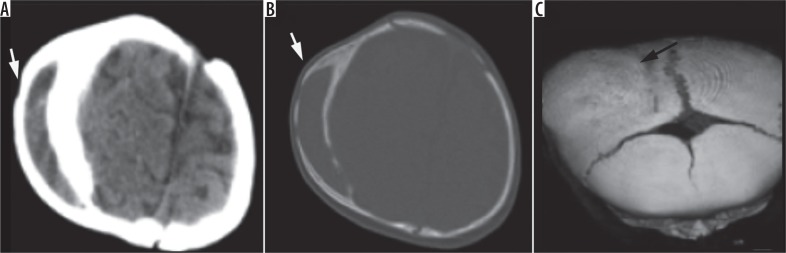
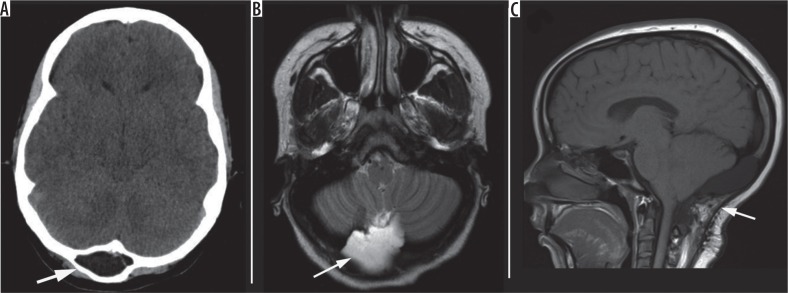
Paediatric skull lesions are commonly identified on imaging. They can be challenging to image, given their location and size, and often require several imaging modalities to narrow down the differential diagnosis. Accurate diagnosis of these lesions is paramount because the clinical therapy can vary tremendously. In this review, we provide a simple and systematic approach to clinical-radiological features of primary skull lesions. We highlight the imaging characteristics and differentiate pathologies based on imaging appearances. We also accentuate the role of cross-sectional imaging in lesion identification and management implications.
Keywords: computed tomography; cross-sectional; magnetic resonance imaging; paediatric skull; skull lesions.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
























Similar articles
-
Calvarial lesions: a radiological approach to diagnosis.Acta Radiol. 2009 Jun;50(5):531-42. doi: 10.1080/02841850902795274. Acta Radiol. 2009. PMID: 19353343 Review.
-
Skull Base Tumors and Tumor-Like Lesions: A Pictorial Review.Pol J Radiol. 2017 Jul 25;82:398-409. doi: 10.12659/PJR.901937. eCollection 2017. Pol J Radiol. 2017. PMID: 28811848 Free PMC article. Review.
-
Skull Imaging-Radiographs and CT revisited.Neurol India. 2020 Jul-Aug;68(4):732-740. doi: 10.4103/0028-3886.293481. Neurol India. 2020. PMID: 32859809 Review.
-
Large solitary lytic skull vault lesions in adults: radiological review with pathological correlation.Clin Imaging. 2020 Feb;59(2):129-143. doi: 10.1016/j.clinimag.2019.10.011. Epub 2019 Nov 27. Clin Imaging. 2020. PMID: 31816540 Review.
-
Spectrum of lytic lesions of the skull: a pictorial essay.Insights Imaging. 2018 Oct;9(5):845-856. doi: 10.1007/s13244-018-0653-y. Epub 2018 Sep 19. Insights Imaging. 2018. PMID: 30232766 Free PMC article. Review.
Cited by
-
Diagnostic Challenge in Rapidly Growing Langerhans Cell Histiocytosis with Aneurysmal Bone Cyst in the Maxilla: A Case Report.Diagnostics (Basel). 2022 Feb 3;12(2):400. doi: 10.3390/diagnostics12020400. Diagnostics (Basel). 2022. PMID: 35204491 Free PMC article.
-
Imaging approach to pediatric calvarial bulges.Pediatr Radiol. 2024 Sep;54(10):1603-1617. doi: 10.1007/s00247-024-05967-9. Epub 2024 Jun 28. Pediatr Radiol. 2024. PMID: 38940907 Review.
-
Isolated infantile myofibroma of the calvarium: Report of a case with a literature review.Childs Nerv Syst. 2024 Apr;40(4):1277-1284. doi: 10.1007/s00381-024-06289-9. Epub 2024 Jan 15. Childs Nerv Syst. 2024. PMID: 38224363 Review.
-
Point-of-care Ultrasound to Distinguish Subgaleal and Cephalohematoma: Case Report.Clin Pract Cases Emerg Med. 2021 May;5(2):198-201. doi: 10.5811/cpcem.2021.3.51375. Clin Pract Cases Emerg Med. 2021. PMID: 34437004 Free PMC article.
-
Pediatric focal calvarial lesions: an illustrated review.Pediatr Radiol. 2023 Dec;53(13):2699-2711. doi: 10.1007/s00247-023-05795-3. Epub 2023 Nov 15. Pediatr Radiol. 2023. PMID: 37964037 Review.
References
-
- Dupuis O, Silveira R, Dupont C, et al. Comparison of “instrument associated” and “spontaneous” obstetric depressed skull fractures in a cohort of 68 neonates. Am J Obstet Gyencol. 2005;192:165–170. - PubMed
-
- Guha-Ray DK. Intrauterine spontaneous depression of fetal skull: a case report and review of literature. J Reprod Med. 1976;16:321–324. - PubMed
-
- Tavares LA, Kottamasu SR, Ezhuthacha SG, et al. Neonatal skull depression: review of four cases. J Perinatol. 1989;9:423–426. - PubMed
-
- Tibbs RE, Lee DC, Parent AD. Depressed skull fracture. In: Batjer HH, Loftus CM, editors. Textbook of Neurological Surgery: Principles and Practice. Philadelphia: Lippincott Williams and Wilkins; 2003. pp. 1082–1095.
-
- Sunil K, Agrawal DM, Praveen Kumar DM, et al. Congenital depression of the skull in neonate: a case of successful conservative management. J Child Neurol. 2010;25:387–389. - PubMed
Publication types
LinkOut - more resources
Full Text Sources