

Research Methods and Progress of Patellofemoral Joint Kinematics: A Review
- PMID: 31019669
- PMCID: PMC6451817
- DOI: 10.1155/2019/9159267
Research Methods and Progress of Patellofemoral Joint Kinematics: A Review
Abstract
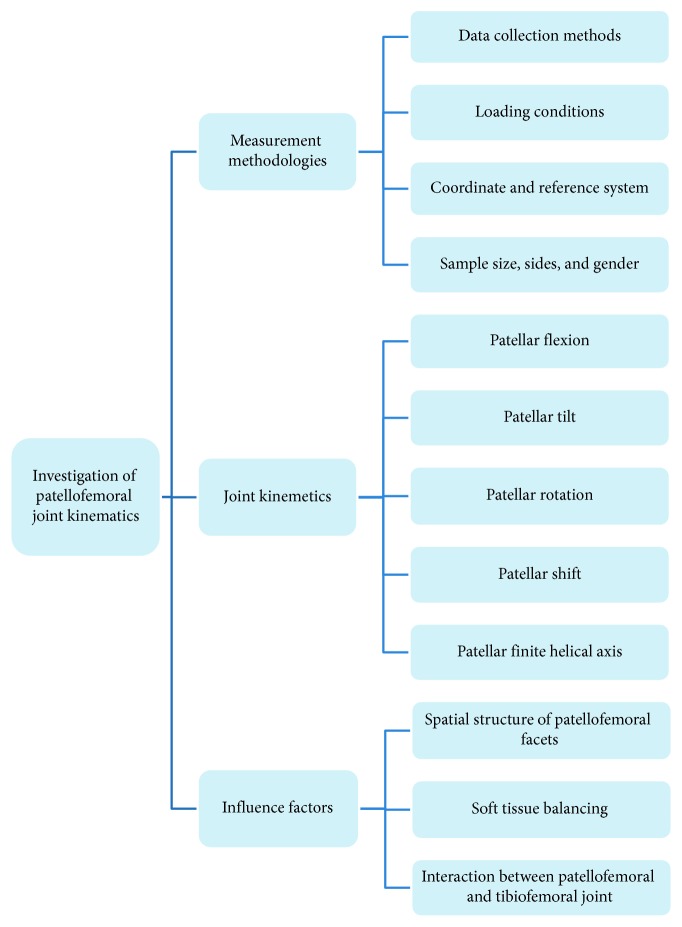
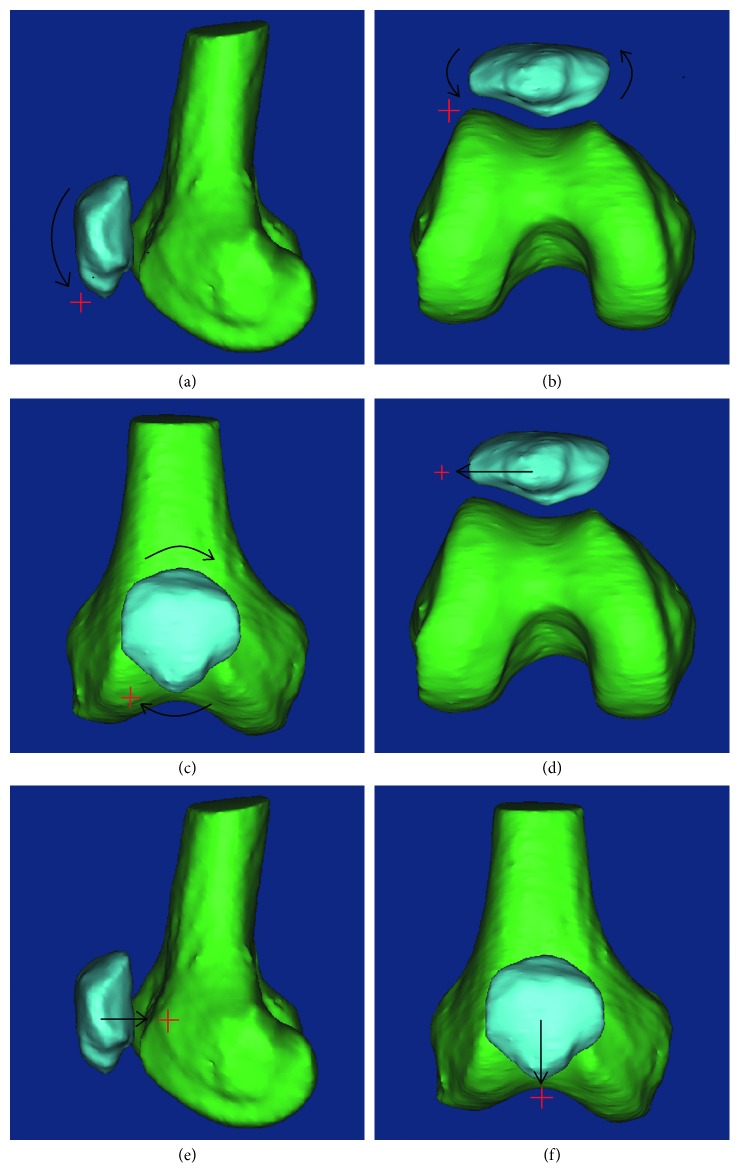
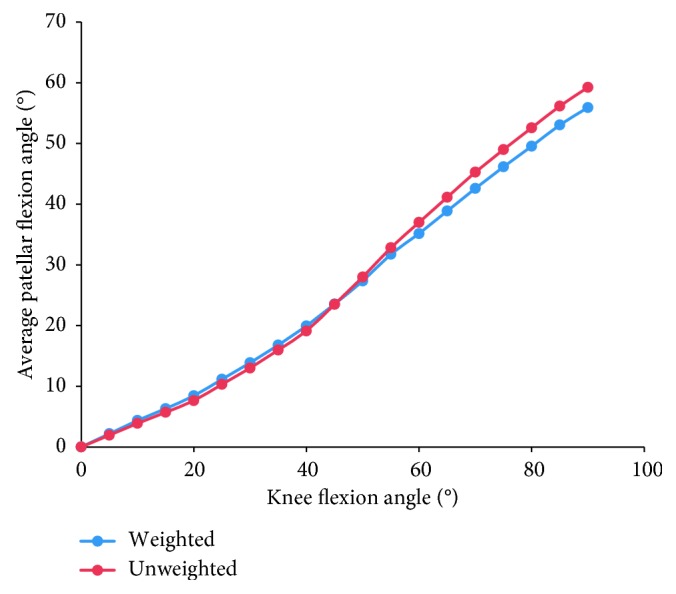
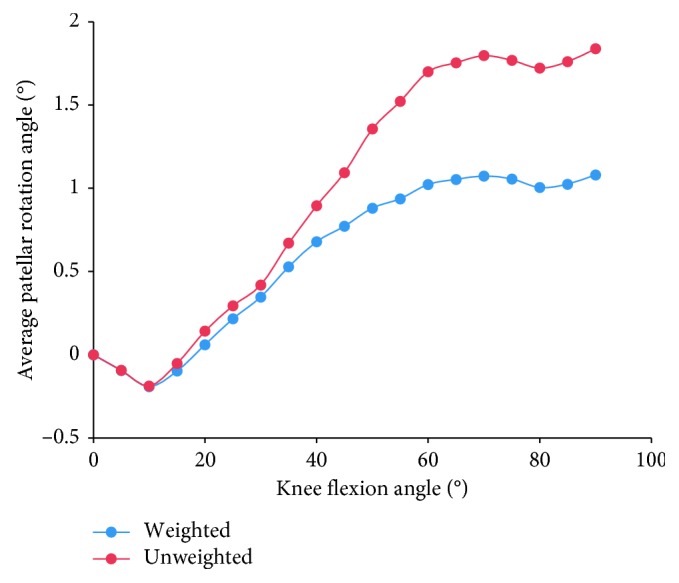
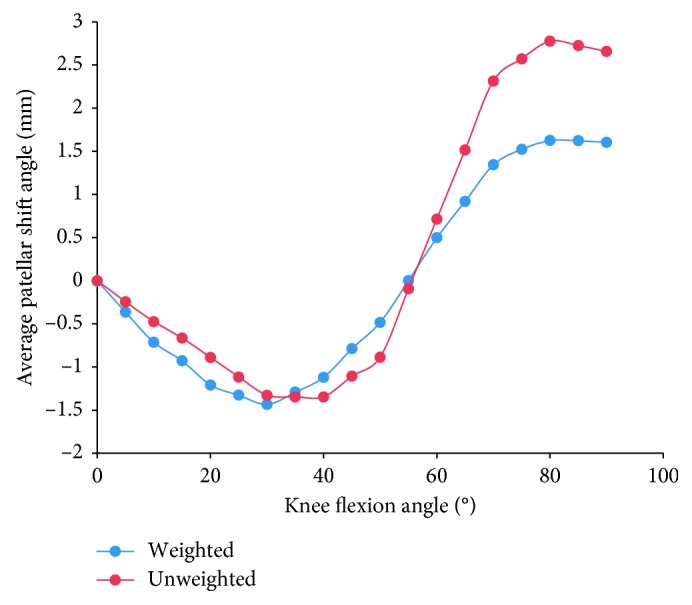
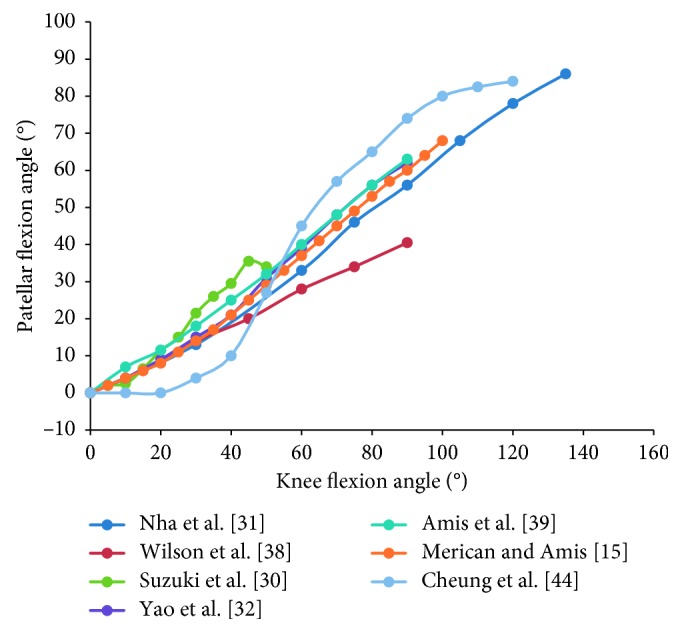
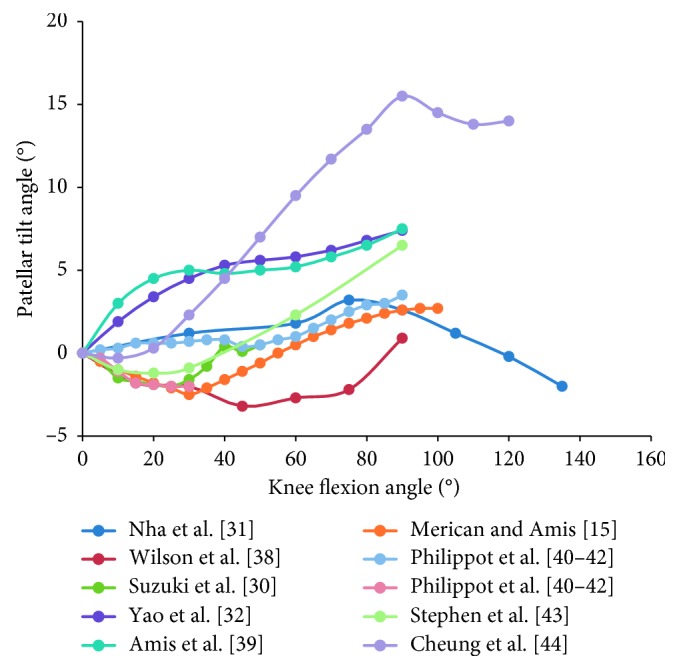
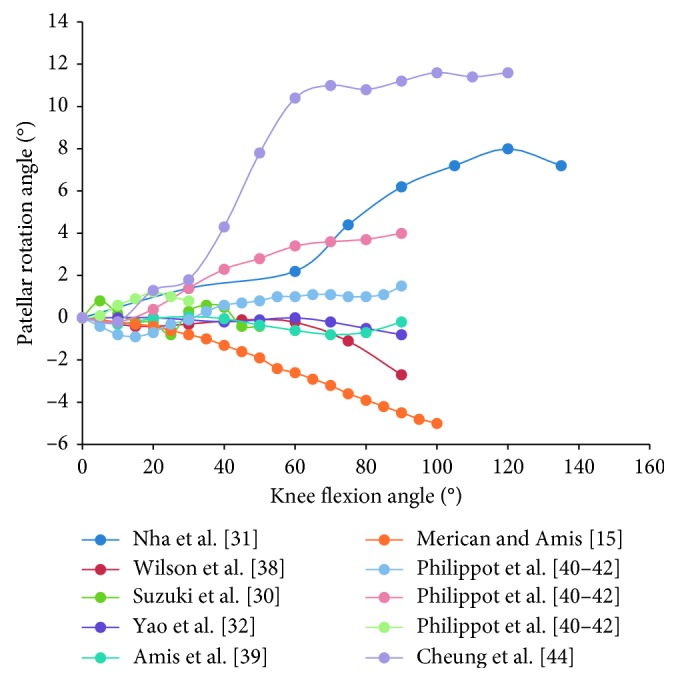
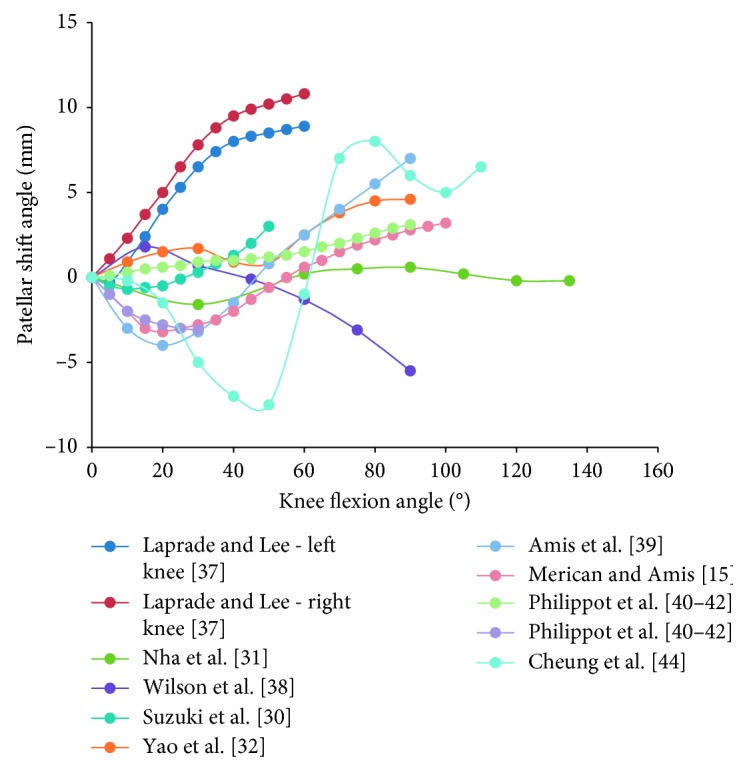
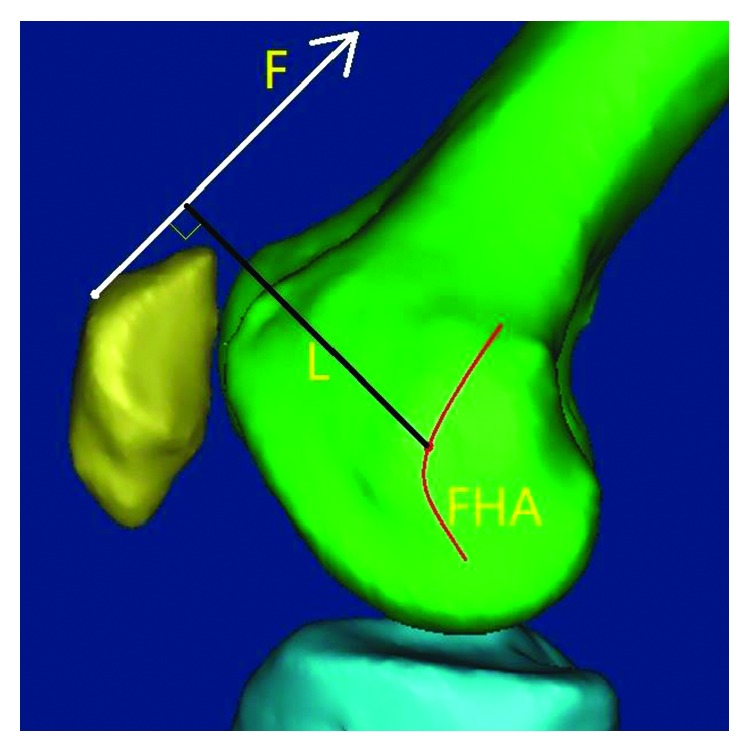
Patellofemoral pain syndrome has a high morbidity, and its pathology is closely associated with patellofemoral joint kinematics. A series of in vivo and in vitro studies have been conducted to explore patellofemoral kinematics, and the findings are relevant to the diagnosis, classification, and management of patellofemoral diseases and even the whole knee joint. However, no definite conclusion on normal patellofemoral kinematics has been established. In this study, the measurement methodologies of patellofemoral kinematics (including data collection methods, loading conditions, and coordinate system) as well as their advantages and limitations were reviewed. Motion characteristics of the patella were analyzed. During knee flexion, the patellar flexion angle lagged by 30-40% compared to the tibiofemoral joint flexion. The patella tilts, rotates, and shifts medially in the initial stage of knee flexion and subsequently tilts, rotates, and shifts laterally. The finite patellar helical axis fluctuates near the femoral transepicondylar axis or posterior condylar axis. Moreover, factors affecting kinematics, such as morphology of the trochlear groove, soft tissue balance, and tibiofemoral motion, were analyzed. At the initial period of flexion, soft tissues play a vital role in adjusting patellar tracking, and during further flexion, the status of the patella is determined by the morphology of the trochlear groove and patellar facet. Our findings could increase our understanding of patellofemoral kinematics and can help to guide the operation plan for patients with patellofemoral pain syndrome.
Figures

Similar articles
-
Tibiofemoral and patellofemoral joint 3D-kinematics in patients with posterior cruciate ligament deficiency compared to healthy volunteers.BMC Musculoskelet Disord. 2012 Nov 26;13:231. doi: 10.1186/1471-2474-13-231. BMC Musculoskelet Disord. 2012. PMID: 23181354 Free PMC article.
-
Patellofemoral arthroplasty influences tibiofemoral kinematics: the effect of patellar thickness.Knee Surg Sports Traumatol Arthrosc. 2014 Oct;22(10):2560-8. doi: 10.1007/s00167-014-3160-9. Epub 2014 Jul 15. Knee Surg Sports Traumatol Arthrosc. 2014. PMID: 25023661
-
Relationship between Patellar Tracking and the "Screw-home" Mechanism of Tibiofemoral Joint.Orthop Surg. 2016 Nov;8(4):490-495. doi: 10.1111/os.12295. Orthop Surg. 2016. PMID: 28032709 Free PMC article.
-
Development of an innovative measurement method for patellar tracking disorder.Aging (Albany NY). 2020 Dec 1;13(1):516-524. doi: 10.18632/aging.202161. Epub 2020 Dec 1. Aging (Albany NY). 2020. PMID: 33260153 Free PMC article. Review.
-
Measurement of patellar tracking: assessment and analysis of the literature.Clin Orthop Relat Res. 2003 Jul;(412):241-59. doi: 10.1097/01.blo.0000068767.86536.9a. Clin Orthop Relat Res. 2003. PMID: 12838076 Review.
Cited by
-
Relationship between patellofemoral finite helical axis and femoral trans-epicondylar axis using a static magnetic resonance-based methodology.J Orthop Surg Res. 2021 Mar 24;16(1):212. doi: 10.1186/s13018-021-02328-2. J Orthop Surg Res. 2021. PMID: 33761974 Free PMC article.
-
The Influence of Mathematical Definitions on Patellar Kinematics Representations.Materials (Basel). 2021 Dec 11;14(24):7644. doi: 10.3390/ma14247644. Materials (Basel). 2021. PMID: 34947239 Free PMC article.
-
Intraoperative Patellofemoral Kinematic Acquisition: The Design, Testing, and Validation of a Setup for Clinical Studies.J Clin Med. 2024 Dec 20;13(24):7784. doi: 10.3390/jcm13247784. J Clin Med. 2024. PMID: 39768708 Free PMC article.
-
Characteristics of the patellofemoral joint of patients with DDH and the effects of Bernese periacetabular osteotomy on the patellofemoral joint.BMC Musculoskelet Disord. 2022 Apr 8;23(1):337. doi: 10.1186/s12891-022-05291-z. BMC Musculoskelet Disord. 2022. PMID: 35395939 Free PMC article.
-
Change in Descriptive Kinematic Parameters of Patients with Patellofemoral Instability When Compared to Individuals with Healthy Knees-A 3D MRI In Vivo Analysis.J Clin Med. 2023 Feb 28;12(5):1917. doi: 10.3390/jcm12051917. J Clin Med. 2023. PMID: 36902705 Free PMC article.
References
-
- Tallay A., Kynsburg A., Toth S., et al. Prevalence of patellofemoral pain syndrome: evaluation of the role of biomechanical malalignments and the role of sport activity. Orvosi Hetilap. 2004;145:2093–2101. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
