

Matrix-Induced Autologous Chondrocyte Implantation With Autologous Bone Grafting for Osteochondral Lesions of the Femoral Trochlea
- PMID: 31019883
- PMCID: PMC6470391
- DOI: 10.1016/j.eats.2018.10.022
Matrix-Induced Autologous Chondrocyte Implantation With Autologous Bone Grafting for Osteochondral Lesions of the Femoral Trochlea
Abstract
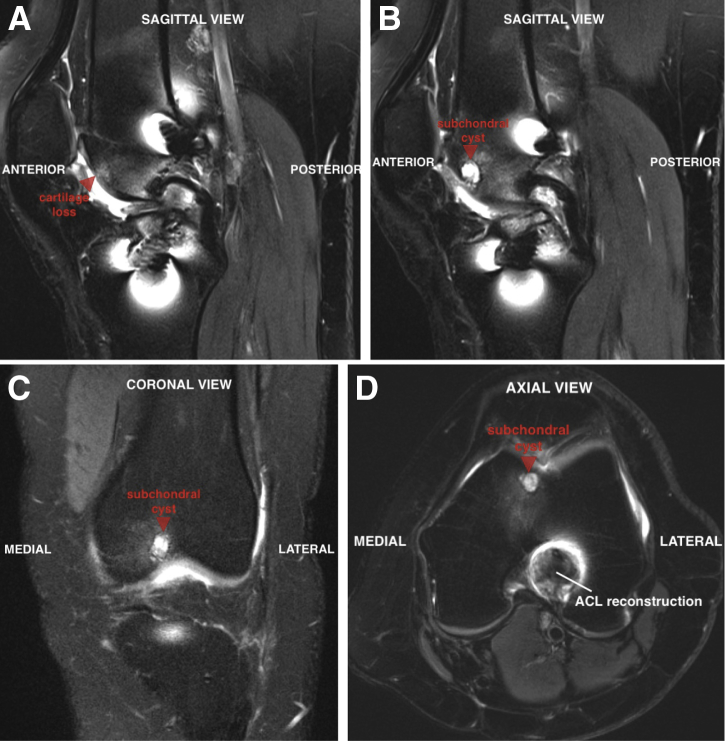
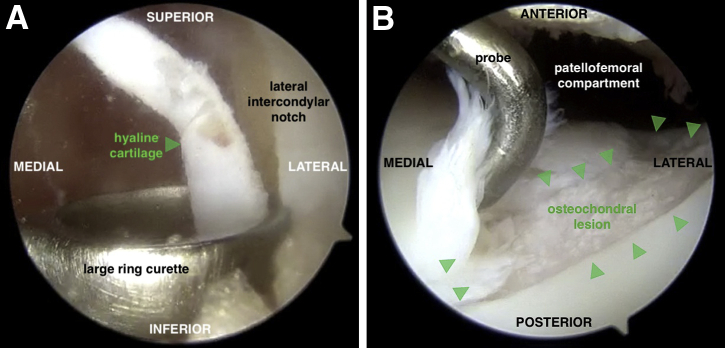
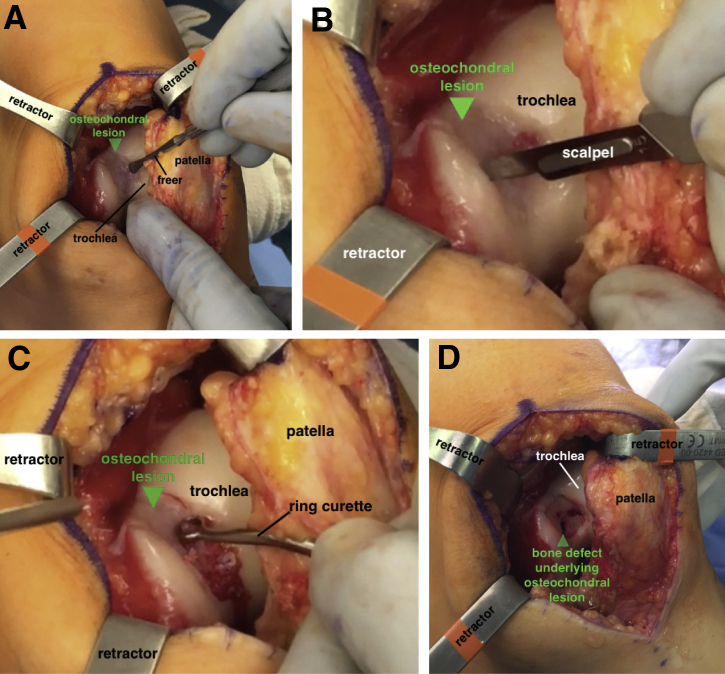
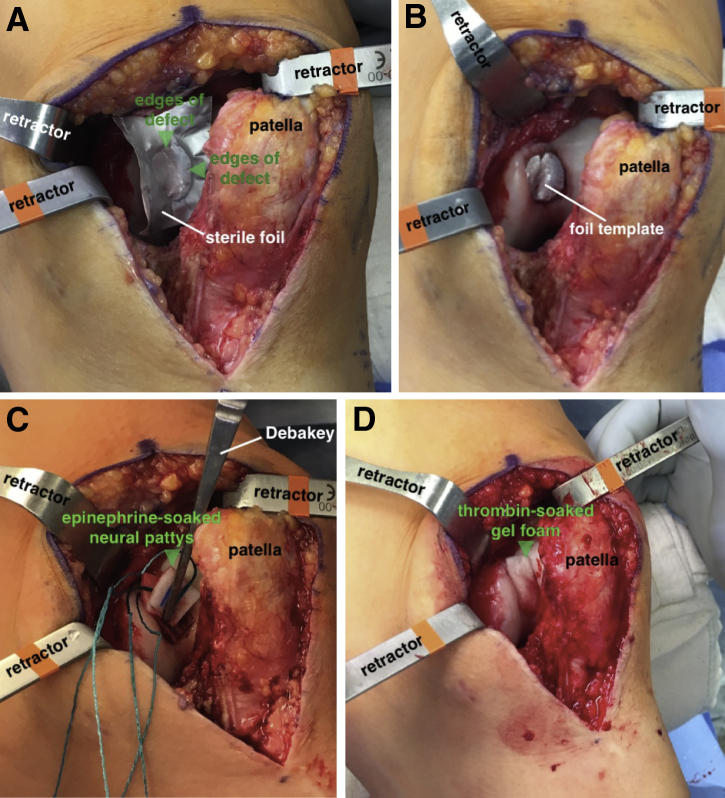
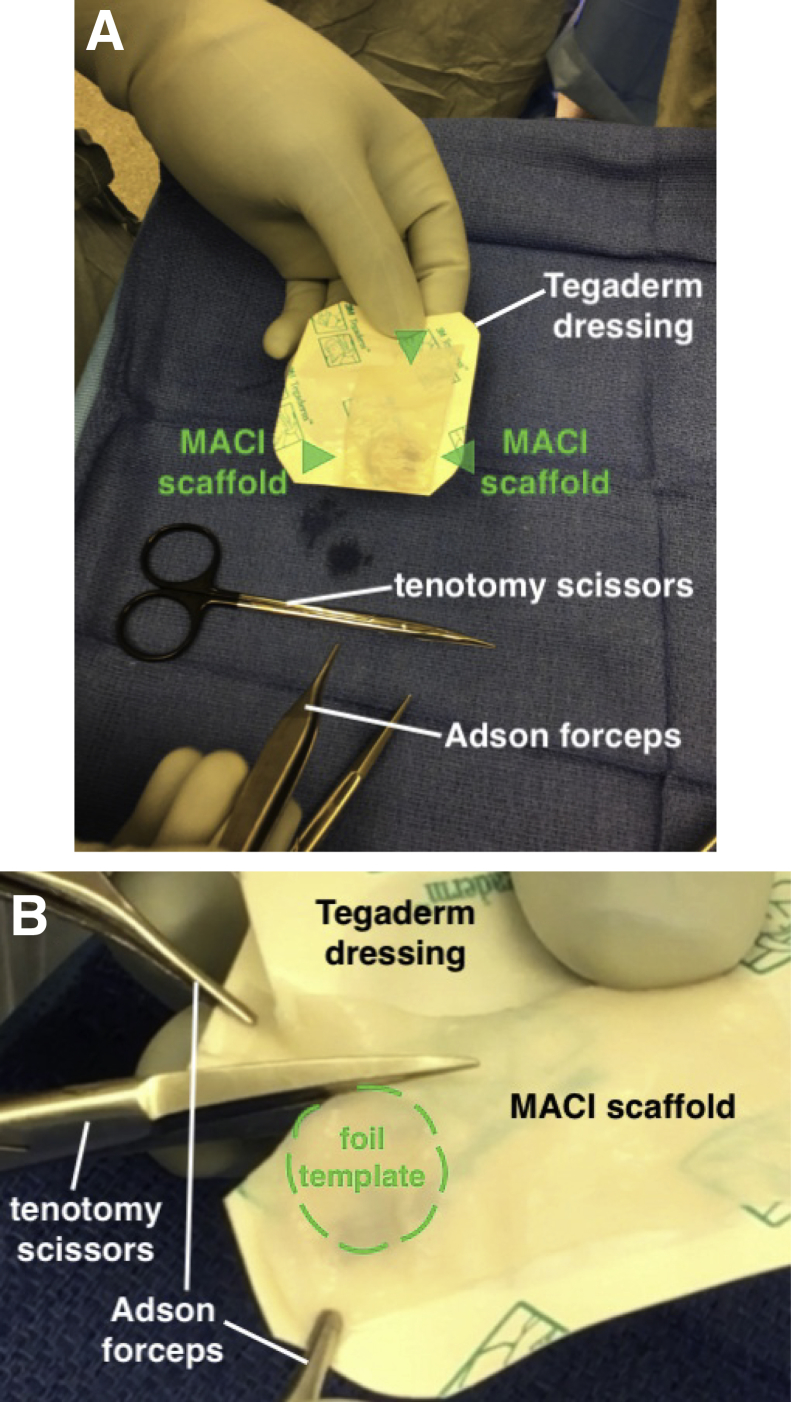
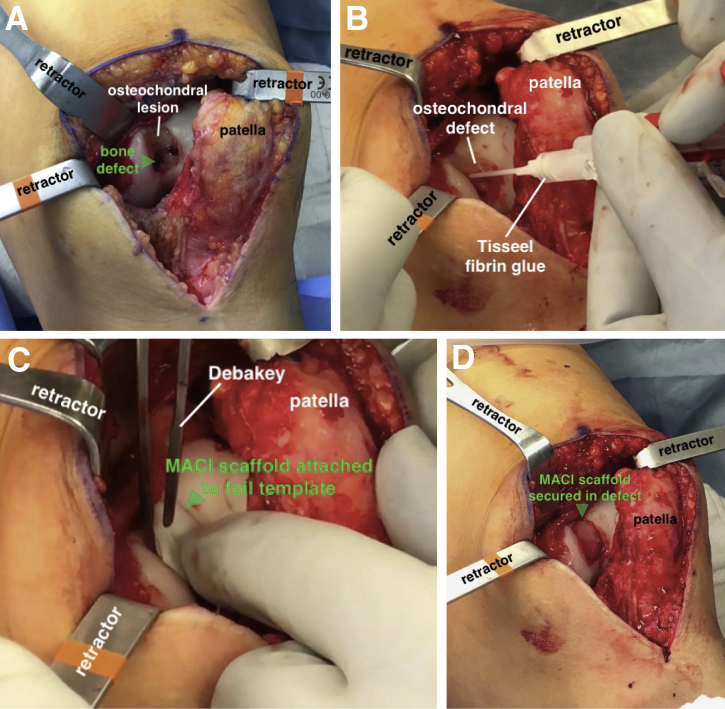
Matrix-induced autologous chondrocyte implantation is a 2-stage surgical procedure used to treat symptomatic, full-thickness chondral lesions of the knee. This third-generation autologous chondrocyte implantation (ACI) technique improves on the limitations of previous methods, including the risk of uneven chondrocyte distribution at the time of implantation and graft hypertrophy. Given the compliant properties of the scaffold, the graft can be easily shaped to treat irregular chondral defects and applied to articular surfaces with multiplanar geometry (e.g., patella, trochlea). Although ACI techniques are ideally suited to treat chondral surface defects, the ACI "sandwich" technique can be used to treat large osteochondral defects with significant bone loss (>8 mm). Historically, this procedure uses autologous bone graft to replace areas of osseous deficiency along with 2 type I/III collagen bilayer membranes to securely contain the cultured chondrocytes within the defect. We present an analogous technique for the treatment of osteochondral lesions of the femoral trochlea using a single matrix-induced ACI scaffold and autologous bone grafting for a segmental osseous defect.
Figures
References
-
- McCormick F., Harris J.D., Abrams G.D. Trends in the surgical treatment of articular cartilage lesions in the United States: An analysis of a large private-payer database over a period of 8 years. Arthroscopy. 2014;30:222–226. - PubMed
-
- Krill M., Early N., Everhart J.S., Flanigan D.C. Autologous chondrocyte implantation (ACI) for knee cartilage defects: A review of indications, technique, and outcomes. JBJS Rev. 2018;6:e5. - PubMed
-
- Brittberg M., Recker D., Ilgenfritz J., Saris D.B.F., SUMMIT Extension Study Group Matrix-applied characterized autologous cultured chondrocytes versus microfracture: Five-year follow-up of a prospective randomized trial. Am J Sports Med. 2018;46:1343–1351. - PubMed
-
- Marlovits S., Aldrian S., Wondrasch B. Clinical and radiological outcomes 5 years after matrix-induced autologous chondrocyte implantation in patients with symptomatic, traumatic chondral defects. Am J Sports Med. 2012;40:2273–2280. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
