

Arthroscopic Knotless Remplissage for the Treatment of Hill-Sachs Lesions Using the PASTA Bridge Configuration
- PMID: 31019885
- PMCID: PMC6471291
- DOI: 10.1016/j.eats.2018.11.001
Arthroscopic Knotless Remplissage for the Treatment of Hill-Sachs Lesions Using the PASTA Bridge Configuration
Abstract
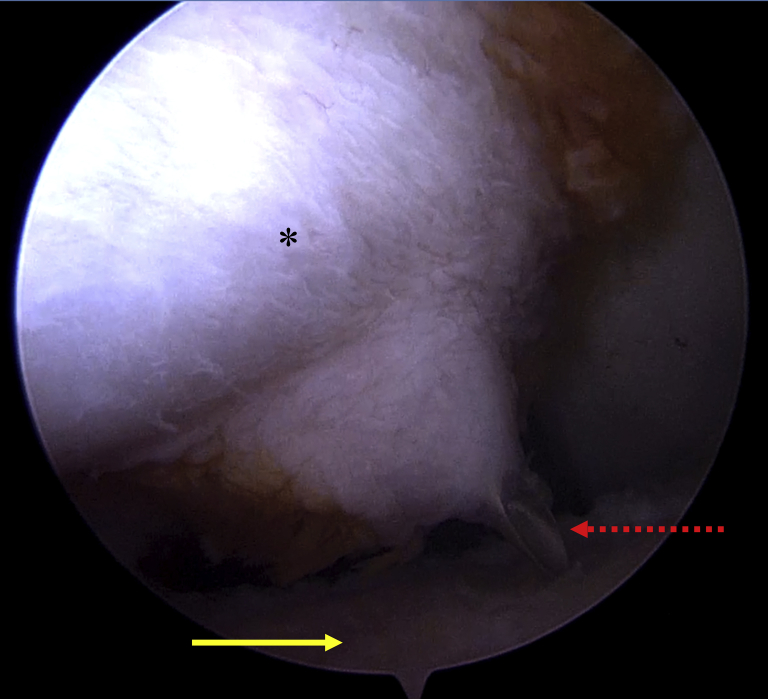
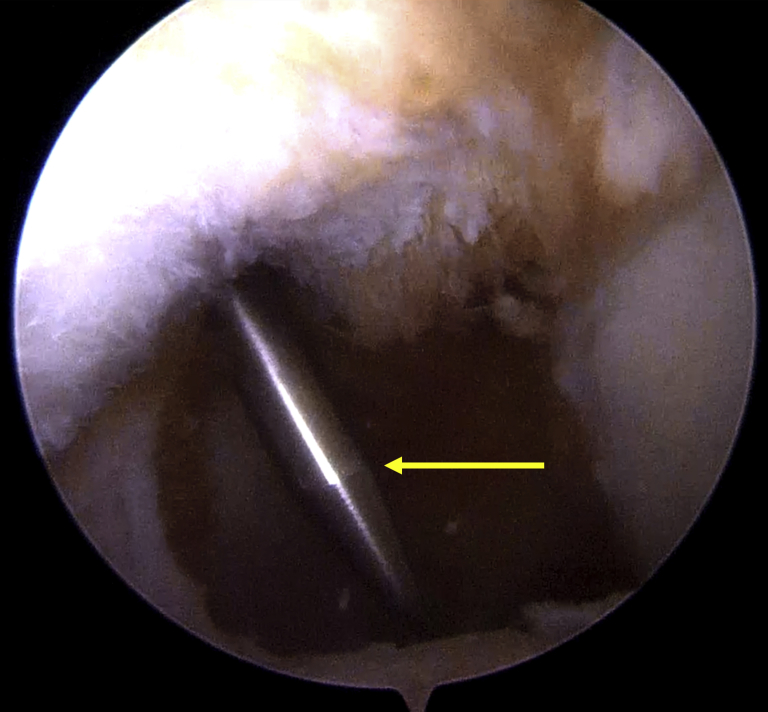
Recurrent glenohumeral dislocations can produce Hill-Sachs lesions-bony defects on the humeral head resulting from the humerus hitting the glenoid during dislocations. Some of these lesions can engage on the glenoid during motion, producing instability and potentially affecting the success of a labral repair. The remplissage was developed to address these Hill-Sachs lesions and improve stability. French for "filling," the goal of the remplissage is to fill the Hill-Sachs lesion with the infraspinatus tendon, preventing the margins of the lesion from engaging with the glenoid. Analogous to restoring the rotator cuff footprint during repair, a primary goal of the remplissage is to have the infraspinatus cover the Hill-Sachs lesion. The partial articular supraspinatus tendon avulsion (PASTA) bridge was originally developed for partial-thickness rotator cuff repair in situ, but additional uses have been found in other settings. The PASTA bridge uses a medial row horizontal mattress with a lateral anchor to create a linked construct to effectively distribute force and provide adequate coverage of the lesion. Knotless anchor technology used in this procedure prevents the need for arthroscopic knot tying and potentially damaging knot stacks. This Technical Note describes a remplissage technique using the PASTA bridge configuration to address Hill-Sachs lesions associated with recurrent glenohumeral instability.
Figures












Similar articles
-
Anterior Shoulder Instability: To Remplissage or Not to Remplissage.Video J Sports Med. 2025 May 20;5(3):26350254241312923. doi: 10.1177/26350254241312923. eCollection 2025 May-Jun. Video J Sports Med. 2025. PMID: 40400711 Free PMC article.
-
Arthroscopic Bankart repair with and without arthroscopic infraspinatus remplissage in anterior shoulder instability with a Hill-Sachs defect: a randomized controlled trial.J Shoulder Elbow Surg. 2021 Jun;30(6):1288-1298. doi: 10.1016/j.jse.2020.11.013. Epub 2020 Dec 26. J Shoulder Elbow Surg. 2021. PMID: 33373683 Clinical Trial.
-
Anatomical and functional results after arthroscopic Hill-Sachs remplissage.J Bone Joint Surg Am. 2012 Apr 4;94(7):618-26. doi: 10.2106/JBJS.K.00101. J Bone Joint Surg Am. 2012. PMID: 22488618
-
[Arthroscopic treatment of Hill-Sachs lesions in glenohumeral instability. "Remplissage" technique].Acta Ortop Mex. 2014 Nov-Dec;28(6):382-8. Acta Ortop Mex. 2014. PMID: 26016292 Review. Spanish.
-
Management of off-track Hill-Sachs lesions in anterior glenohumeral instability.J Exp Orthop. 2023 Mar 21;10(1):30. doi: 10.1186/s40634-023-00588-x. J Exp Orthop. 2023. PMID: 36943508 Free PMC article. Review.
Cited by
-
Arthroscopic All-Inside Remplissage Technique With Knotless Tape Bridge for Hill-Sachs Lesions.Arthrosc Tech. 2023 Aug 7;12(9):e1487-e1494. doi: 10.1016/j.eats.2023.04.021. eCollection 2023 Sep. Arthrosc Tech. 2023. PMID: 37780647 Free PMC article.
References
-
- Skendzel J.G., Sekiya J.K. Diagnosis and management of humeral head bone loss in shoulder instability. Am J Sports Med. 2012;40:2633–2644. - PubMed
-
- Weber B.G., Simpson L.A., Hardegger F. Rotational humeral osteotomy for recurrent anterior dislocation of the shoulder associated with a large Hill-Sachs lesion. J Bone Joint Surg Am. 1984;66:1443–1450. - PubMed
-
- Armitage M.S., Faber K.J., Drosdowech D.S., Litchfield R.B., Athwal G.S. Humeral head bone defects: Remplissage, allograft, and arthroplasty. Orthop Clin N Am. 2010;41:417–425. - PubMed
-
- Saltzman B.M., Riboh J.C., Cole B.J., Yanke A.B. Humeral head reconstruction with osteochondral allograft transplantation. Arthroscopy. 2015;31:1827–1834. - PubMed
-
- Kazel M.D., Sekiya J.K., Greene J.A., Bruker C.T. Percutaneous correction (humeroplasty) of humeral head defects (Hill-Sachs) associated with anterior shoulder instability: A cadaveric study. Arthroscopy. 2005;21:1473–1478. - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
